


![Opioids Agonists : Clinical uses
These are used as analgesic agents. Visceral, dull and
constant pain is relieved more effectively than inflammatory
pain. Opioids are however contraindicated in biliary colic.
Morphine (i.v.) is useful in myocardial infarction as well as in
acute pulmonary edema.
Codeine, pholcodeine, dextromethorphan and noscapine are
effective cough suppressants. Dextromethorphan is devoid of
constipating action unlike other drugs in this group.
Loperamide and diphenoxylate can be used for the treatment
of non-infective diarrhea.
Morphine is useful as a pre-anaesthetic medication whereas
highly lipid soluble drugs (like fentanyl, alfentanil, sufentanil
etc) are used as adjuncts to other anaesthetic agents.
Pethidine is used to reduce shivering after anaesthesia [by its
action on a2 receptor]](https://image.slidesharecdn.com/opioidanalgesicsandantagonists-201005030541/85/Opioid-analgesics-and-antagonists-10-320.jpg)



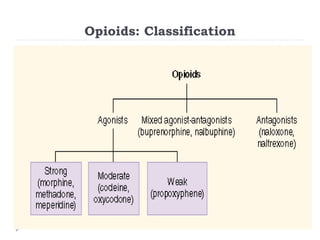
This document summarizes opioids and their mechanisms of action. It discusses that opioids act on mu, kappa, and delta opioid receptors in the central nervous system and gastrointestinal tract to produce analgesia, euphoria, sedation and other effects. The document outlines the classification, agonists, antagonists and effects of different opioid receptors. It provides details on commonly used opioid analgesics like morphine, codeine, methadone, tramadol and their indications, pharmacological actions, and adverse effects. Peripheral opioid antagonists are discussed for treating opioid-induced constipation.
















































































