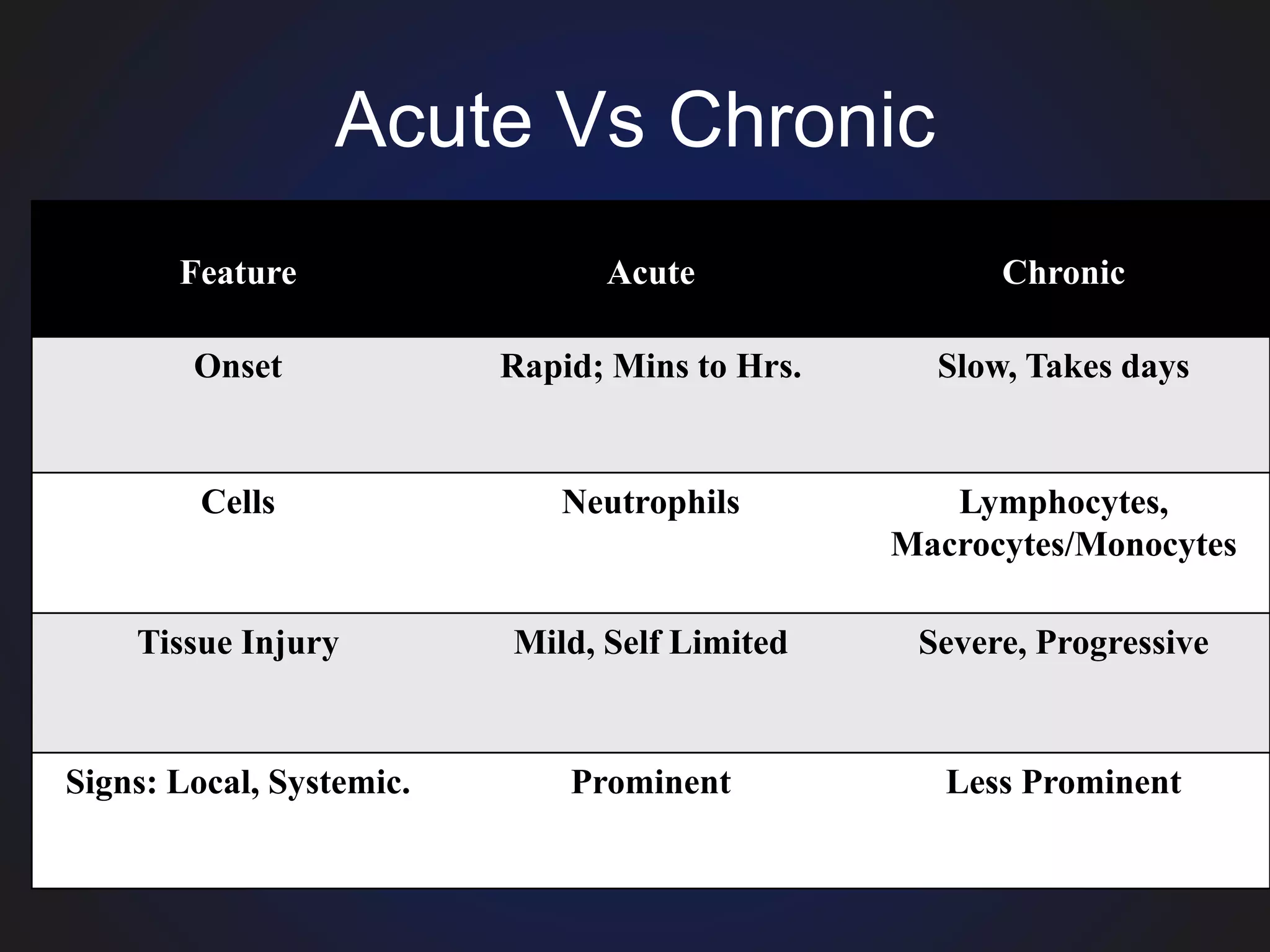
Inflammation is the body's response to injury or infection. It involves vascular changes that increase blood flow to the injured area, allowing immune cells and proteins to be delivered. The immune cells migrate into tissues and remove the injurious agent through phagocytosis. The process is tightly regulated to resolve inflammation and repair tissue damage. The cardinal signs of inflammation are redness, swelling, heat, pain, and loss of function. Acute inflammation typically involves neutrophils and resolves within a few weeks, while chronic inflammation involves lymphocytes and can cause progressive tissue damage.





















































































![Inflammation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/inflammationautosaved-180806124543-thumbnail.jpg?width=640&height=640&fit=bounds)






















































