OBSTRUCTIVE JAUNDICE
It isthe jaundice that develops due to biliary obstruction partial or
complete or intermittent
It causes conjugated hyperbiliruminemia
Normal Serum bilirubin level is 0.2-0.8mg%
Scleral icterus is visible when Serum bilirubin level exceeds
2.5mg%
3.
CAUSES OF OBSTRUCTIVEJAUNDICE
1. Congenital: Biliary atresia, choledochal
cyst.
2. Inflammatory: Ascending cholangitis,
sclerosing cholangitis.
3. Obstructive: CBD stones, biliary stricture,
parasitic infestation.
4. Neoplastic: Carcinoma of head or
periampullary region of pancreas,
cholangiocarcinomas, Klatskin tumour.
5. Extrinsic compression of CBD by
lymph nodes or tumours.
4.
CLINICAL FEATURES
Jaundice:
1.Onset
- usually gradual in most cases
- May be sudden in conditions like cholidocholithiasis
2. Duration
- persistent if due to malignancy ( Cholangiocarcinomas, periampullary
carcinoma, head of pancreas carcinoma)
- intermittent or waxing or wanning if related to stone related
obstruction or biliary stricture
3.Progression
- progression worsening of jaundice over days to weeks suggestive of
malignancy
- Sudden onset with rapid progression may indicate CBD stones or
biliary obstruction
5.
Pain
Painless jaundice :
carcinomaof head of pancreas- continuous and progressive
dull constent right upper quadrant /epigastric region
Periampullary carcinoma – intermittent (due to sloughing of
tumour)
Painful jaundice:
CBD stones- intermittent colicky type of pain
Fever
cholangitis – whether associated with chills and rigors
more come in case of stone disease rather than
malignancy . Charcot’s triad ( seen in ascending cholangitis)
- intermittent Fever, pain, jaundice
6.
Pruritis:
All over thebody – As a result of bile flow obstruction bile salts
deposited in the hair follicles of skin causes irritation of nerve ending
situated in the dermis
weight loss
Loss of appetite
vomiting - More likely present in CBD stones , cholangitis ,
periampullary carcinoma
Dark coloured urine
Passing clay coloured stools
Steatorrhoea
Breathlessness,cough, hemoptysis
Headache,seizures,dizziness
7.
Signs
jaundice- seenin sclera and skin
Scratch marks – seen over arms,chest,abdomen,back
Hepatomegaly
Palpable gallbladder : - Murphy’s sign
- Moynihan’s method
- courvoisiers law – if there is palpable gallbladder it is not due
to stones .
1. Mucocele
2.Empyema
3.obstructive jaundice due to carcinoma pancreas
4. Carcinoma of gallbladder
8.
Signs ofliver cell failure
Stigmata of malignancy- Cachexia , lymphadenopathy- virchow’s node, sister Mary Joseph
nodule, ascites.
Cholelithiasis
gall stones – most common type of stone mixed stone
Types of stones :
* Cholesterol stones (Cholesterol solitaire-radiating crystalline
appearance) are 6% common, often solitary.
* Mixed stones are 90% common. It contains cholesterol,
calcium salts of phosphate carbonate
*Pigment stones are small, black or greenish black, multiple.
Often they can be sludge like.
*Common in “Fat, Fertile, Forty, Flatulent, Female”.
Pathogenesis : Lithogenic bile, nucleation, stasis
9.
Infections and Infestations:
-Bacteria like E. Coli, Salmonella
- Parasites like Clonorchis sinensis and Ascaris lumbricoides are often
associated.
- Moynihan’s aphorism:“A gallstone is a tomb stone
erected to the memory of the organism within it.”
Bile stasis:
, - Occurs due to estrogen therapy, pregnancy, vagotomy
and in patients who are on long-term intravenous fluids
or TPN.
Increased bilirubin production
- Due to any of the causes of haemolysis as in hereditary
spherocytosis, sickle cell anaemia, thalassaemia, malaria,
cirrhosis. Here pigment stones are common.
10.
Complication :
In thegall bladder:
• Acute cholecystitis
• Chronic cholecystitis
• Mucocele
• Empyema
• Gangrene
• Carcinoma
• Fistula
In the CBD : Secondary CBD stones (occurs in 10% of gallstones).
Cholangitis.
Pancreatitis.
Mirizzi syndrome (compression of CHD/CBD by stone
from cystic duct or cholecysto-choledochal fistula).
11.
Mirizzi Syndrome :
• It refers to the obstruction or stricture of the common
hepatic duct as result extrinsic Compression by a gallstone in the
hartmann’s pouch
Types:
• Type 1 (11%): Extrinsic compression of CHD by a large stone in
Hartmann’s pouch
• Type 2 (41%): Stone has now eroded into the hepatic duct to form
a fistula involving less than 1/3rd
of circumference
• Type 3 (44%): Lesions involve 2/3rd
of circumference
• Type 4 (<4%): Completely destroyed hepatic duct.
12.
Cholecystoenteric Fistula
• Mostcommon site duodenum
• Diagnosis suspicious by presence
of air in bile duct
• Complication—gallstone ileus
• Other sites fistula—colon.
Saints triad
• Gallstones
• Diverticulosis of colon
• Hiatus of hernia
Spread ;
-Direct spread to liver (segment IV and V), bile duct,
duodenum, colon and kidney.
-Lymphatic-lymph node of Lund, periportal nodes, peripancreatic and periduodenal nodes.
-Blood spread-to liver, lungs and bones.
- Perineural spread is also known to occur.
Features of Carcinoma gallbladder;
• Pain in right hypochondrium, mass in right upper abdomen
which is hard and nontender (gallbladder
•Significant weight loss in short duration, anorexia
•Acute presentation of cholecystitis.
•Palpable nodular liver secondaries, ascites.
•Incidentally confirmed by histological report as carcinoma gallbladder after
cholecystectomy for chronic cholecystitis.
Three clinical presentations: (1) Clinically obvious type with pain, obstructive jaundice, mass.
(2) cancer mimics GB stone disease. (3) Atypical as unusual features.
16.
Prognosis
Overall prognosisfor carcinoma gallbladder is poor due
to
early spread and aggressive nature of the tumour.
5-year survival is only 5%. Muscle invasion, nodal and
distant spread carry poor prognosis. In stage T1 simple and
extended cholecystectomy will not make difference in
prognosis. In T2, stage extended cholecystectomy is very much
beneficial which gives 60% 5-year survival rate.T3 and T4 carry
poor prognosis
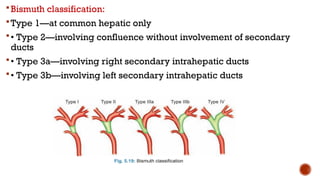
Bismuth classification:
Type 1—atcommon hepatic only
• Type 2—involving confluence without involvement of secondary
ducts
• Type 3a—involving right secondary intrahepatic ducts
• Type 3b—involving left secondary intrahepatic ducts
19.
Klatskin tumour:
-It is cholangiocarcinoma at the confluence of the
hepatic
ducts and common hepatic duct above the level of the cystic
duct (20% of cholangiocarcinomas).
- Klatskin tumour is classified as 4 types-I: Just at or below
the confluence; II: At the confluence; Ill: At the confluence
extending along the RHO; IV: At the confluence extending
along the LHD.
- It causes obstructive jaundice with hydrohepatosis without
enlargement of gallbladder.
20.
Case scenario
A 62-year-oldfemale presented with a 2-weekhistory
of progressive yellow discoloration of the eyes and
skin, associated with itching,dark-colored urine, and pale
stoolsShe also reports dull, aching pain in the right upper
abdomen for 3 days, with decreased appetite and weight
loss.There is no history of fever, vomiting, oraltered sensorium.
She is a known diabetic onregular medication On examination,
she is icteric, with scratchmarks visible over her limbs.
Abdominal examination revealed mild tenderness in the right
hypochondrium and a palpable gallbladder.There is no
hepatosplenomegaly