Download as PDF, PPTX
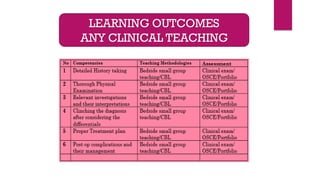
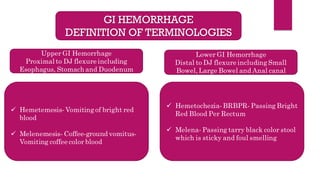
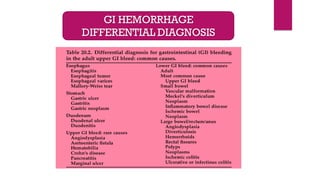
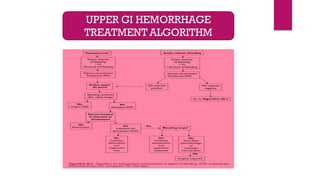
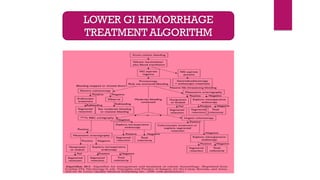
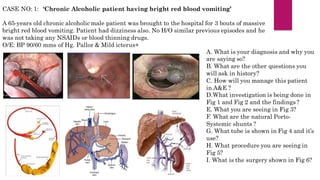


This document presents clinical vignettes related to gastrointestinal (GI) hemorrhage, including definitions of key terminologies such as hematemesis and melena. It discusses various case scenarios involving patients with different GI bleeding presentations, their evaluations, diagnoses, and management strategies. The document emphasizes the importance of differential diagnosis and investigations for effective patient management in emergency settings.























































































