Downloaded 131 times


























![PREDISPOSING FACTORS
Pre-existing renal impairment [> 1.5 mg/dl], particularly when
secondary to diabetic nephropathy.
Large doses of contrast media and multiple injections within
72 h.
The route of administration (IA > IV).
Dehydration and CHF. Hypertension, hyperuricemia and
prteinuria. Multiple Myeloma.
Nephrotoxic drugs.
Type of CM.](https://image.slidesharecdn.com/conventionalnephroradiology-170414212010/85/Conventional-nephroradiology-72-320.jpg)


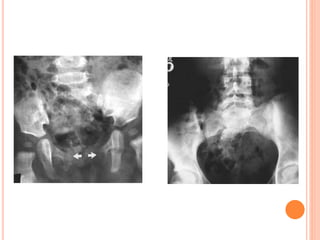

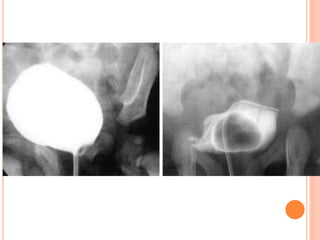

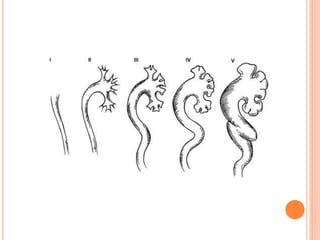



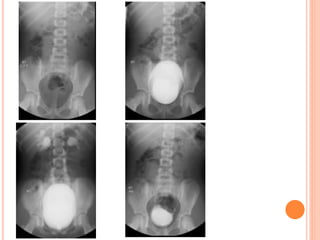

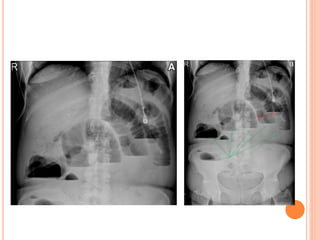




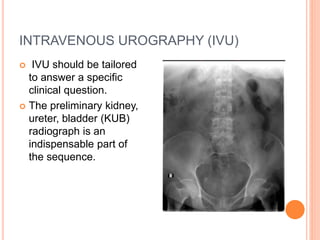
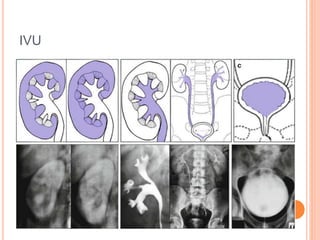
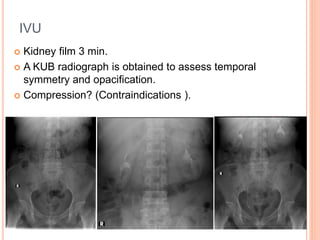
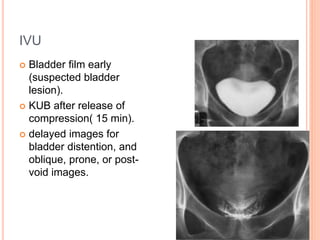
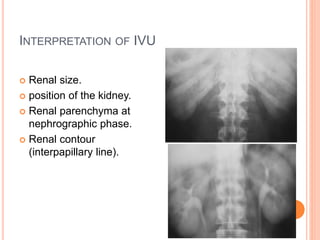
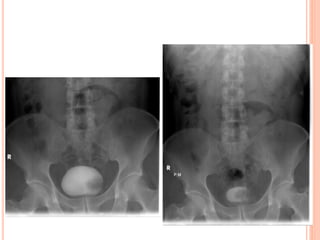
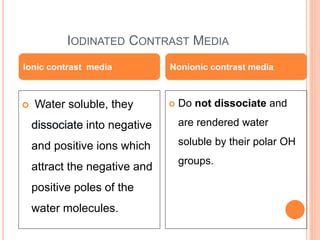
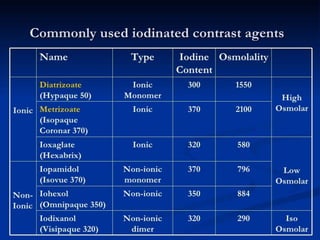
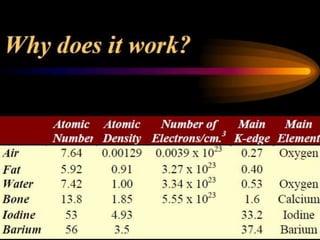
The document provides an overview of conventional imaging techniques of the urinary tract. It discusses conventional radiography, intravenous urography (IVU), voiding cystourethrography (VCUG), and contrast media. IVU involves injecting contrast dye intravenously to image the kidneys, ureters, and bladder. It allows evaluation of renal size and function. VCUG assesses the bladder, urethra, and detects vesicoureteral reflux by filling the bladder with contrast under fluoroscopy during voiding. The document outlines procedures, interpretations, and risks of these techniques, emphasizing their role in evaluating the urinary system.























































































