Downloaded 50 times







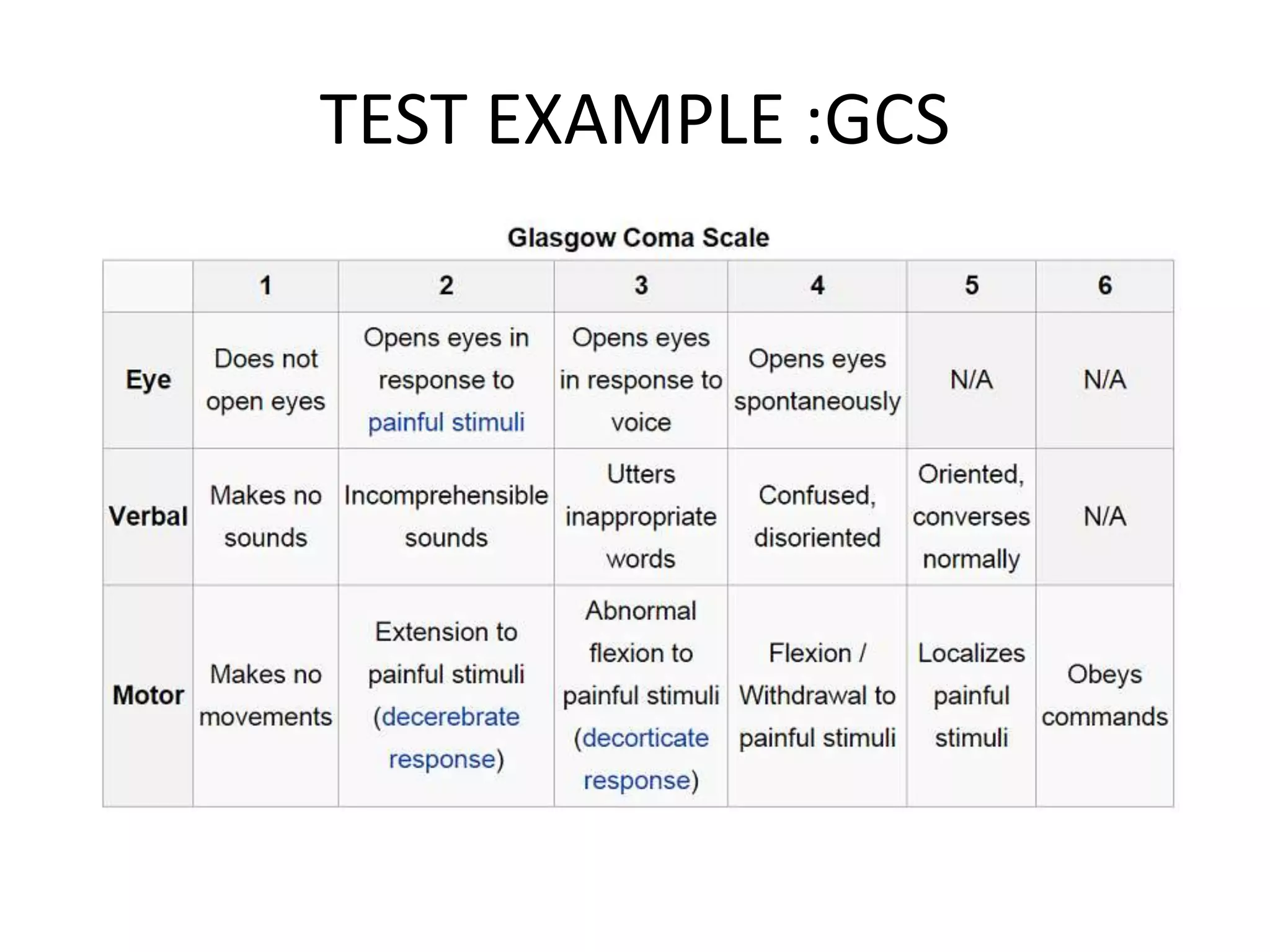













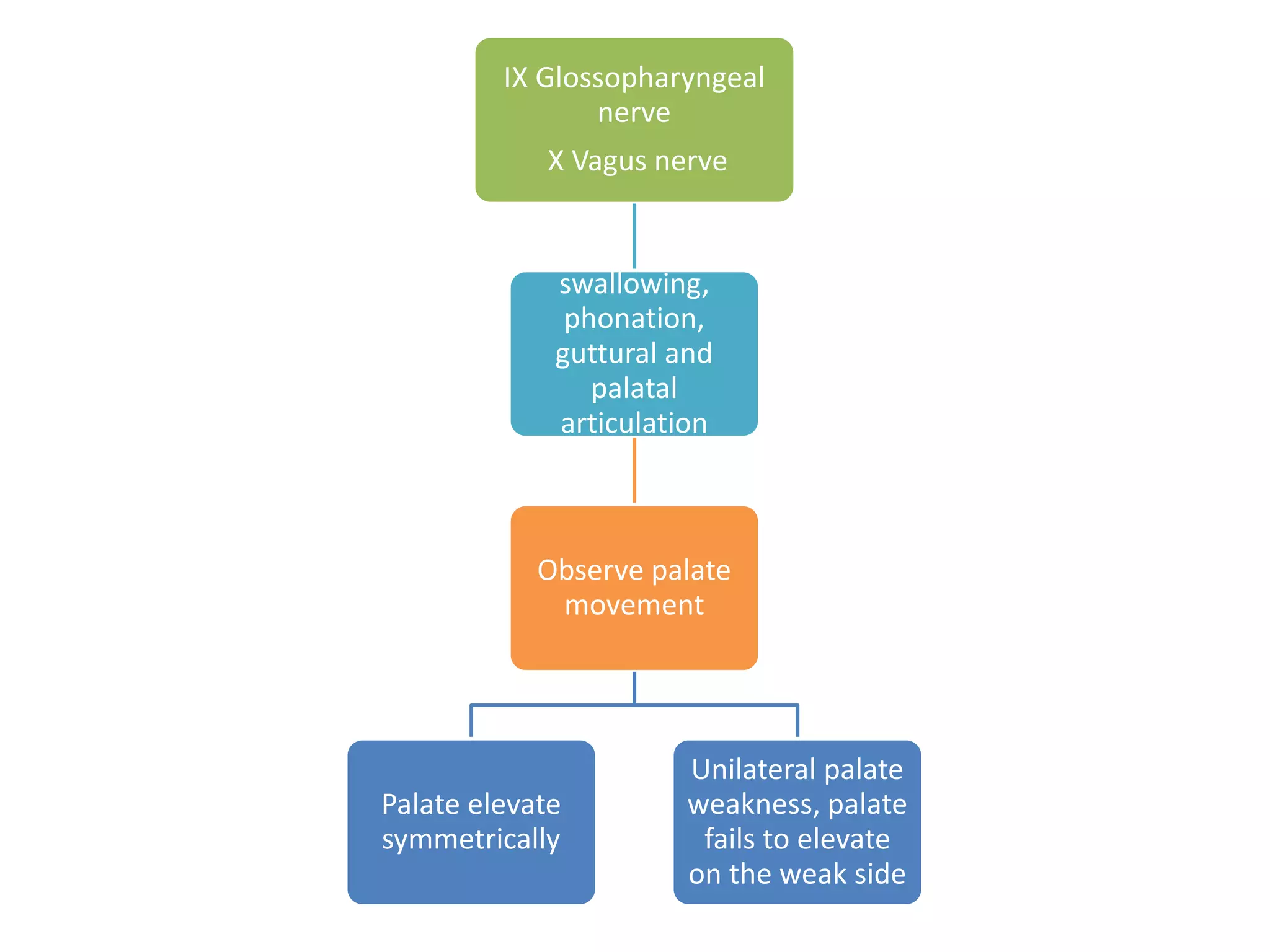







The document provides a comprehensive overview of neurological examinations, detailing various components such as sensory and reflex examinations, mental status assessments, and motor evaluations. It includes specific tests and examples, as well as mnemonics for remembering cranial nerve functions. The text emphasizes the importance of observing patient responses to different stimuli and movements to assess the integrity of the nervous system.