Downloaded 57 times




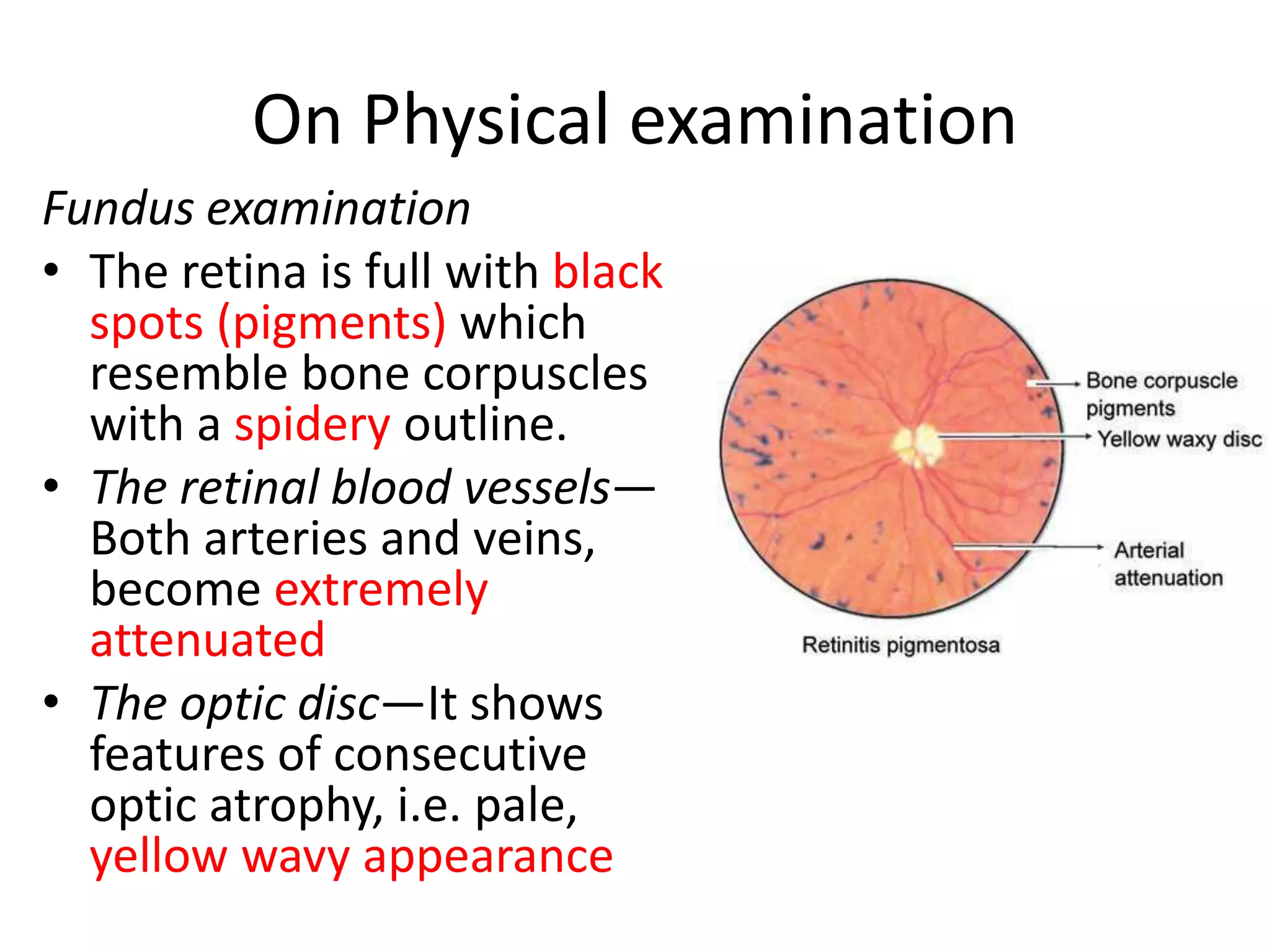






Retinitis pigmentosa is a slow degenerative, hereditary disease of the retina that involves the rods and cones. It typically appears as a recessive trait due to consanguinity of the parents. Patients experience night blindness in childhood, tunnel vision or central visual loss in middle age, and complete blindness in advanced age. Physical examination shows black spots resembling bone corpuscles across the retina, extremely attenuated retinal blood vessels, and pale optic discs, indicating optic nerve atrophy. There is no specific treatment currently available, but cataract surgery and rehabilitation services can help manage complications.























































































