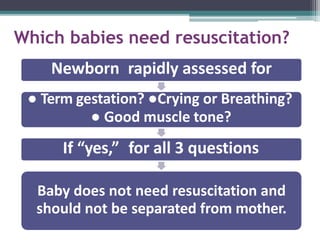
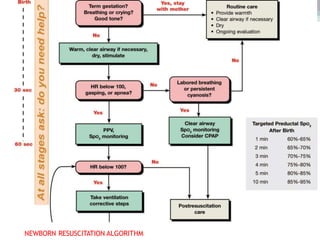
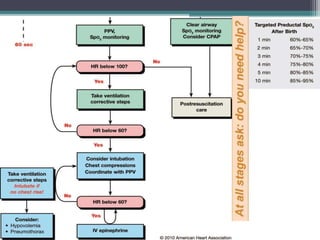
This document provides information on neonatal resuscitation. It discusses assessing newborns at birth to identify those requiring resuscitation, initial resuscitation steps including warming, positioning, clearing airways, drying, and stimulating breathing. It describes providing pulmonary resuscitation through ventilation with oxygen or CPAP and vascular resuscitation including cardiac massage if the heart rate is low. Key equipment, monitoring, temperature control, airway clearance and surfactant administration are outlined. The document emphasizes prompt response and evaluation during resuscitation.













![Neonatal resuscitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/neonatalresuscitationautosaved-210325082037-thumbnail.jpg?width=640&height=640&fit=bounds)




































