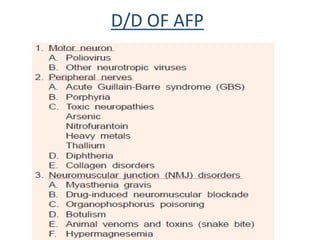
AFP surveillance is critical for global polio eradication. All cases of acute flaccid paralysis in children under 15 are investigated to differentiate between polio and other causes like Guillain-Barre syndrome, transverse myelitis, traumatic neuritis, and post-diphtheritic polyneuropathy. Stool specimens are collected from AFP cases and tested to isolate poliovirus. If wild poliovirus is isolated, the case is confirmed as polio. Surveillance ensures rapid detection of wild poliovirus circulation.