













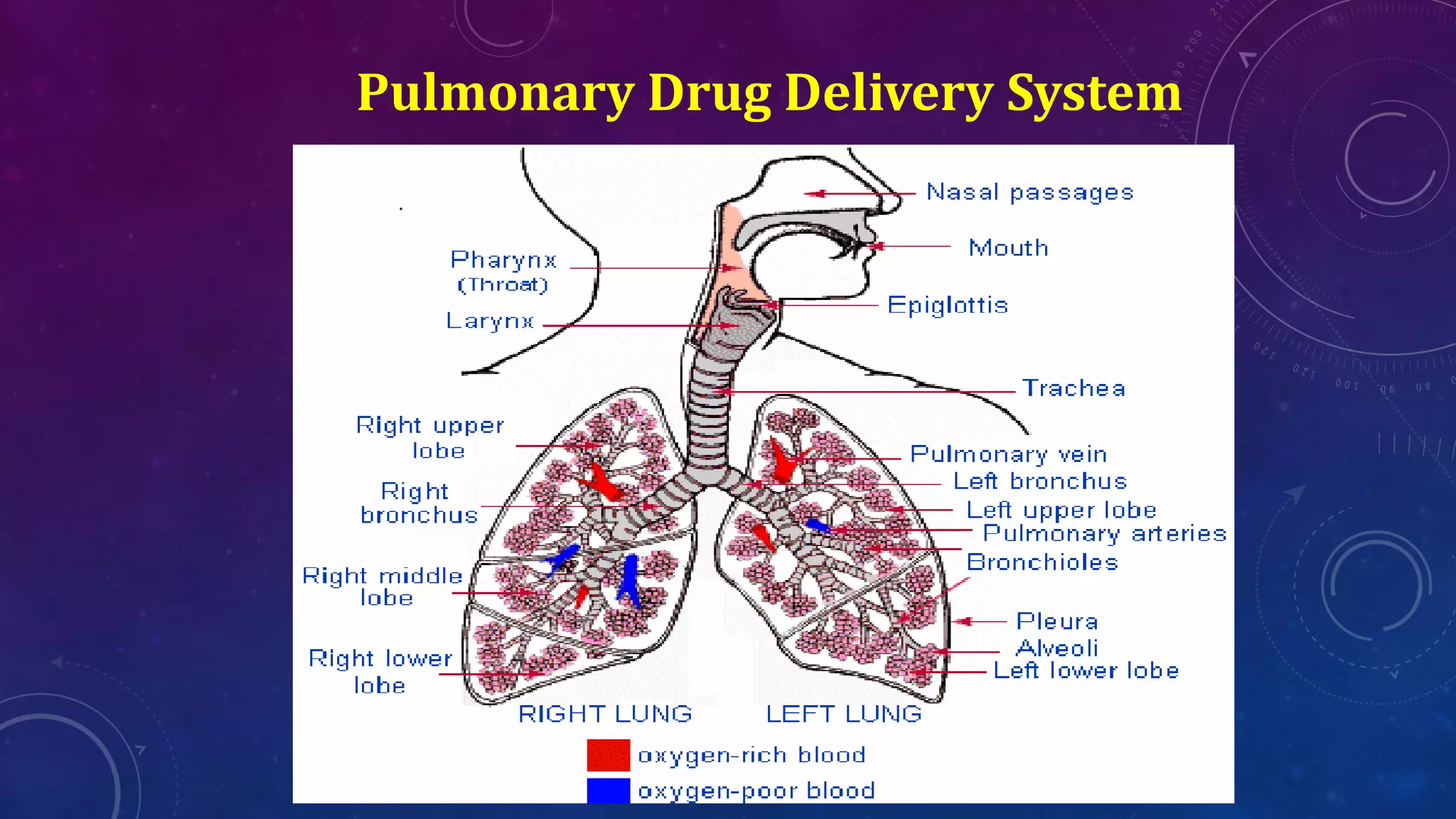












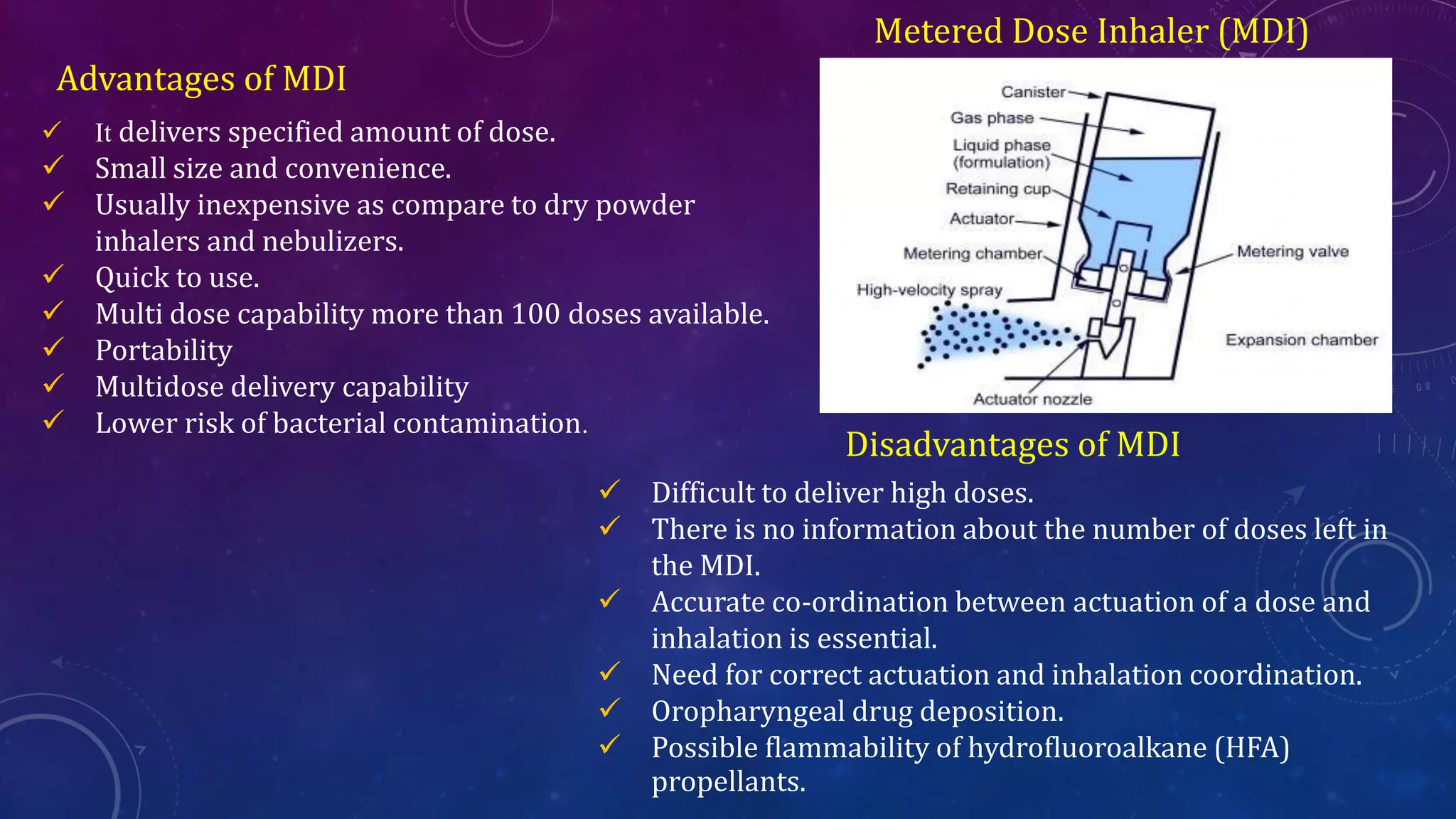




The document provides information on nasopulmonary drug delivery systems including nasal drug delivery and pulmonary drug delivery. It discusses the anatomy and physiology of the nasal cavity and respiratory tract. It also describes various formulation approaches for nasal delivery such as nasal gels, drops, sprays and powders. The document further explains dry powder inhalers, metered dose inhalers and nebulizers as pulmonary drug delivery systems along with their advantages and disadvantages. It also discusses some marketed products for nasal sprays, dry powder inhalers and metered dose inhalers.























































































