Downloaded 284 times
![References 19Acetadote [package insert]. Nashville, TN:Cumberland Pharmaceuticals, Inc.; February 2006.Gurbuz AK, Ozel AM, Ozturk R, Yildirim S, Yazgan Y, Demirturk L. Effect of N-acetyl cysteine on Helicobacter pylori. South Med J. 2005;98:1095-1097Lacy, CF, Armstrong, LL, Goldman, MP, Lance, LL. Drug information handbook.17th ed. Hudson: Lexi-Comp, Inc.; c2008. Acetylcysteine; p. 32-4.N-Acetylcysteine, a Novel Treatment for Helicobacter pylori Infection. Dig Dis Sci. 2004 Nov-Dec;49(11-12):1853-61. Pombrio JM, Giangreco A, Li L, Wempe MF, Anders MW, Sweet DH, Pritchard JB, Ballatori N. Mercapturic acids (N-acetylcysteine S-conjugates) as endogenous substrates for the renal organic anion transporter-1. Mol Pharmacol. 2001 Nov;60(5):1091-9.Up to date online. Prevention of contrast-induced nephropathy. Rudnick, MR, Tumlin, JA. 2009 Sep.Dribben WH, Porto SM, Jeffords BK. Stability and microbiology of inhalant N-acetylcysteine used as an intravenous solution for the treatment of acetaminophen poisoning. Ann Emerg Med. 2003 Jul;42(1):9-13](https://image.slidesharecdn.com/nacetylcysteine-12761281847169-phpapp01/85/N-Acetylcysteine-19-320.jpg)

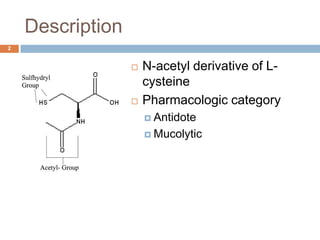
N-acetylcysteine (NAC) is an antidote and mucolytic agent with FDA approval for acetaminophen overdose and adjunctive mucolytic therapy. It works by increasing glutathione stores to prevent liver toxicity from acetaminophen or by lowering mucus viscosity. NAC is available as an intravenous or inhaled solution and oral capsules. The intravenous route is preferred for severe overdose or inability to take oral medications. Common side effects include nausea and vomiting. While its efficacy for other off-label uses like contrast-induced nephrotoxicity prevention is unclear, it is generally well-tolerated with minimal drug interactions.









































![Anticholinergics[1]](https://cdn.slidesharecdn.com/ss_thumbnails/anticholinergics1-141013095608-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)













































