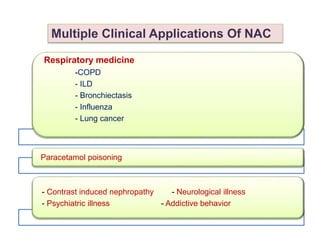
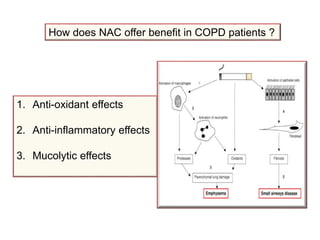
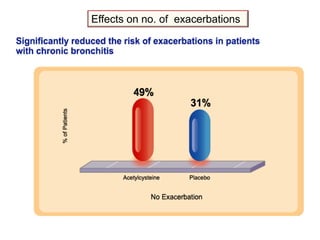
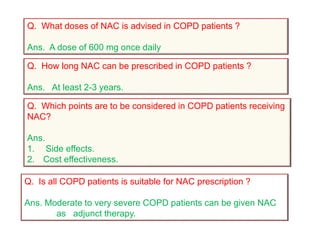
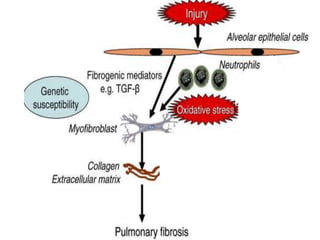
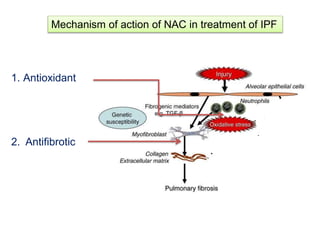
Acetylcysteine (NAC) is a widely used pharmaceutical drug with multiple clinical applications. It has antioxidant and anti-inflammatory properties. NAC is beneficial for COPD by reducing oxidative stress, inflammation, and mucus viscosity. It can slow lung function decline and reduce exacerbations. NAC may also slow disease progression in IPF by reducing fibrosis. In bronchiectasis, NAC helps clear mucus as a mucolytic and can reduce exacerbations. NAC can also reduce the severity and duration of influenza episodes. Some research indicates NAC may help protect normal cells from chemotherapy and radiation used to treat cancers like lung cancer.