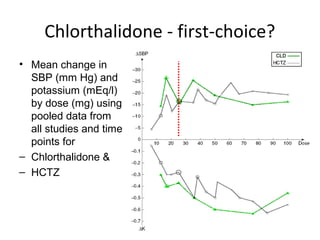
Chlorthalidone has been shown to be more effective at lowering blood pressure than hydrochlorothiazide, especially at night, due to its longer half-life. Evidence from large clinical trials also indicates that chlorthalidone reduces cardiovascular outcomes more than hydrochlorothiazide when used for hypertension. As a result, clinical guidelines now recommend chlorthalidone as the first-line thiazide-type diuretic for treating hypertension.

![Cardiovascular Therapeutics - A
Companion to Braunwald's Heart Disease , 4th Edition
• This is likely because
chlorthalidone has a
longer half life than
HCTZ. [50-60 hours
vs. 9-10 hours]](https://image.slidesharecdn.com/temisartanchlorthalidone-140912011717-phpapp02/85/Temisartan-chlorthalidone-31-320.jpg)





































![Anticholinergics[1]](https://cdn.slidesharecdn.com/ss_thumbnails/anticholinergics1-141013095608-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)





































































