Downloaded 573 times



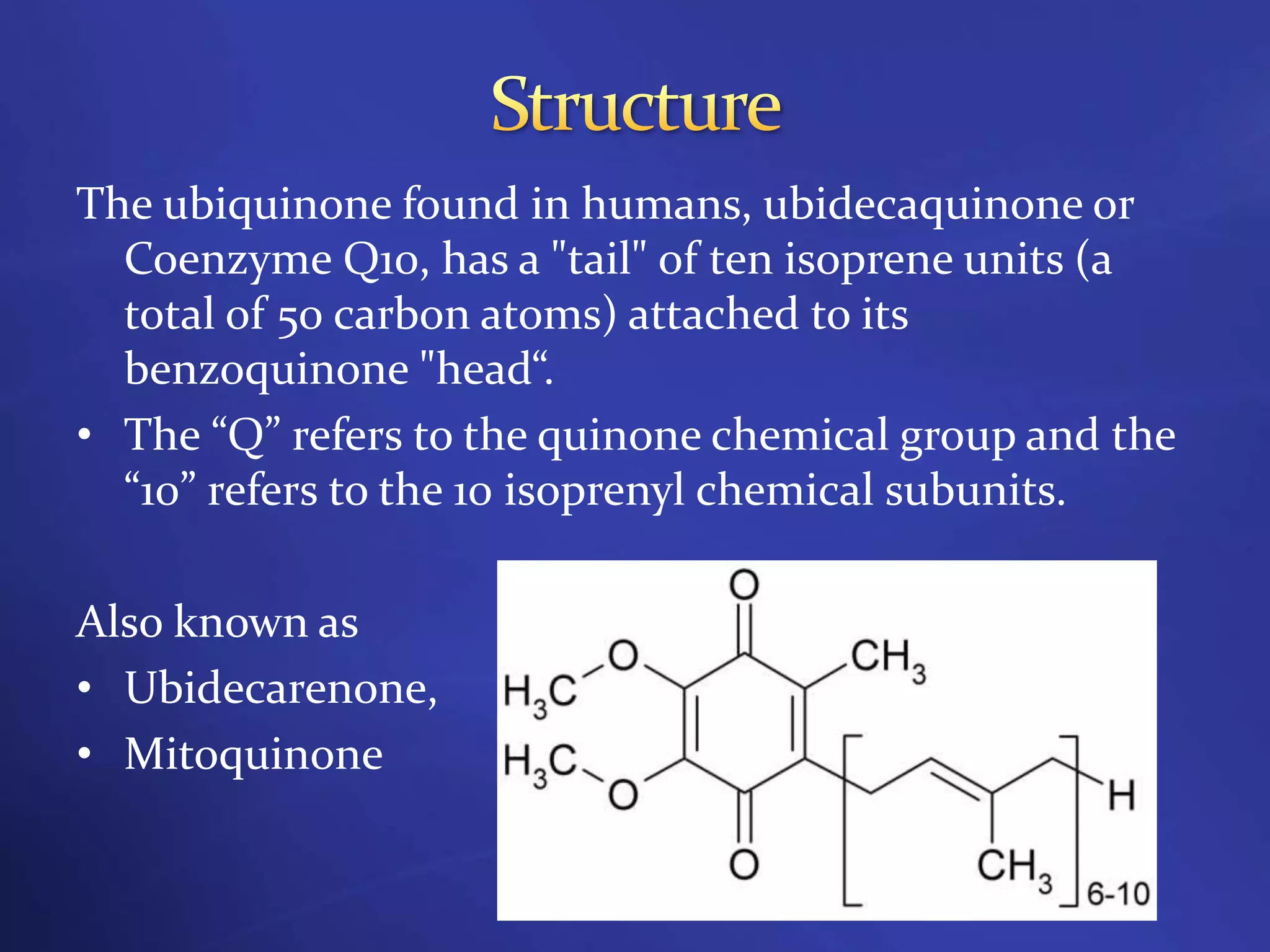


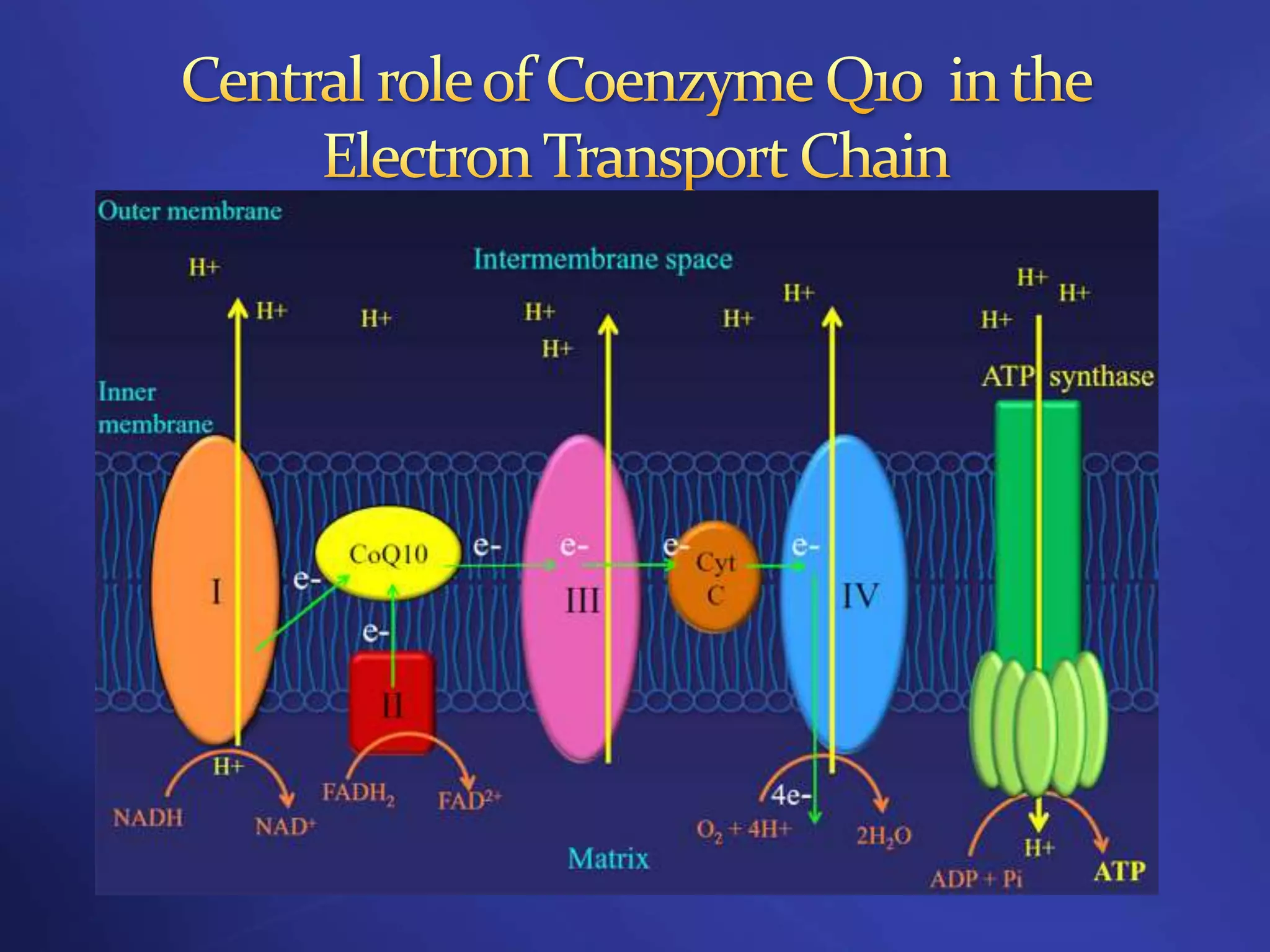





















Coenzyme Q10 is a lipid-soluble antioxidant that is synthesized in the body and functions as a cofactor in ATP synthesis. It accepts and donates electrons during oxidative phosphorylation and also acts as an antioxidant. Due to its roles in energy production and antioxidant properties, Coenzyme Q10 supplementation has shown promise in treating cardiovascular diseases, neurodegenerative diseases, cancer, and diabetes, though more research is still needed to validate its therapeutic benefits.





































![VITAMIN B12[CYNACOBALAMIN][COBALAMIN],SOURCES OFVITAMIN B12,VITAMIN B12 DEFIC...](https://cdn.slidesharecdn.com/ss_thumbnails/vitaminb12ravisankar-vignanpharmacy-130615121944-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































