INTRODUCTION
Paracetamol (UK/International) orAcetaminophen (US) is the generic for N-acetyl-p-
aminophenol (APAP)
The most widely used analgesic and antipyretic in pediatrics
Available in multiple formulations , strengths , combination
Commonly available in any home ,where it can be :
1/Unintentionally ingested by young children ( i.e. <12 yr. )
2/Intentional overdose by adolescents and adults ( i.e. >12 yr.)
3/Inappropriate dosed in all ages
PHARMACOLOGY : THERAPEUTICUSES
APAP Treat fever & Relieve pain
Useful with gastric complaints/risks with NSAIDs
Analgesic/Antipyretic of choice for children with viral infections (Aspirin = Reye Syndrome)
PHARMACOLOGY : PHARMACOKINETICS
APAPmetabolism occur in the liver (conjugation ) to form gluconidated60% and
sulfated30% metabolites (~90%) excreted by urine .
A portion (~5%) of APAP is metabolized via hepatic cytochrome p450 enzyme
CYP2E1 to form N-Acetyl-p-benzoquinoneimine NAPQI a highly reactive intermediate
metabolite that react with sulfhydryl groups .
At normal doses of acetaminophen NAPQI reacts with sulfhydryl group of glutathione
produced by the liver ,forming water soluble mercapturic acid conjugate to be excreted
in urine .
7.
PHARMACOLOGY : ADVERSEEFFECTS
With Large doses of APAP the available glutathione in the liver becomes depleted
and NAPQI reacts with sulfhydryl groups of hepatic proteins causing centrilobular
liver necrosis which can lead to liver failure .
Other causes of decreased glutathione production :
Viral hepatitis or any liver disease
Epilepsy
TB
Fever, dehydration ,malnutrition are also causes of decreased glutathione production.
DOSAGES
Therapeutic dose :
10-15mg/kg Q4-6 hr. , 5 times /day (max.)
MAX. dose : 75 mg/kg/day
Toxicity :
The single acute toxic dose of APAP is >200 mg/kg (150 mg/kg in US/MOH SA
protocol) in children.
- for this patient use Rumack-Matthew nomogram
Repeated Supratherapeutic doses ( >90 mg/kg/24hr. For consecutive days ) can also
lead to hepatic injury/failure in children that have problems with glutathione production
10.
CLINICAL MANIFESTATION
The initialsymptoms are nonspecific (i.e. nausea &vomiting ) and my not be present
Thus the diagnosis of APAP toxicity cannot be based on clinical symptoms alone , but
instead a combination of :
Patient History + Physical Examination + Labs
11.
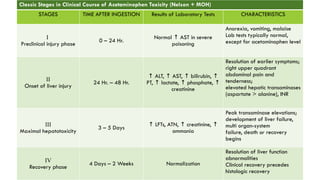
Classic Stages inClinical Course of Acetaminophen Toxicity (Nelson + MOH)
STAGES TIME AFTER INGESTION Results of Laboratory Tests CHARACTERISTICS
I
Preclinical injury phase
0 – 24 Hr.
Normal AST in severe
↑
poisoning
Anorexia, vomiting, malaise
Lab tests typically normal,
except for acetaminophen level
II
Onset of liver injury
24 Hr. – 48 Hr.
↑ ALT, AST, bilirubin,
↑ ↑ ↑
PT, lactate, phosphate,
↑ ↑ ↑
creatinine
Resolution of earlier symptoms;
right upper quadrant
abdominal pain and
tenderness;
elevated hepatic transaminases
(aspartate > alanine), INR
III
Maximal hepatotoxicity
3 – 5 Days
↑ LFTs, ATN, creatinine,
↑ ↑
ammonia
Peak transaminase elevations;
development of liver failure,
multi organ-system
failure, death or recovery
begins
IV
Recovery phase
4 Days – 2 Weeks Normalization
Resolution of liver function
abnormalities
Clinical recovery precedes
histologic recovery
12.
INVESTIGATIONS
RBS + VBG
APAPlevel should by measured after 4 hr. of reported time of ingestion.
LFT
Coagulation profile PT,APTT, INR
KFT
FBC
Serum Lipase
Serum Lactic Acid
13.
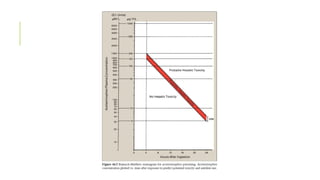
RUMACK-MATTHEW NOMOGRAM
Utilized afteran single acute ingestion to determine if Antidote therapy is needed.
Based on the time of ingestion and the serum acetaminophen level
Levels should be obtained between 4 and 24 hours post ingestion.
Not valid for:
•Unknown ingestion time.
•Repeated supratherapeutic doses.
•Extended-release formulations.
•IV paracetamol.
15.
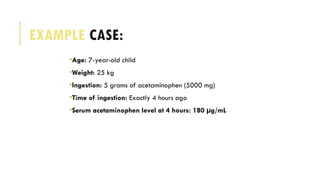
EXAMPLE CASE:
•Age: 7-year-oldchild
•Weight: 25 kg
•Ingestion: 5 grams of acetaminophen (5000 mg)
•Time of ingestion: Exactly 4 hours ago
•Serum acetaminophen level at 4 hours: 180 µg/mL
16.
TREATMENT
Patient poisoned orpotentially poisoned :
1/ABCs
2/Activated Charcoal : 1 gram/kg (max ~50–100 g)
3/Place the patient into one of the following four categories:
1.Prohylactic
2.Hepatic injury
3.Acute liver failure
4.Repeated supratherapeutic ingestion
17.
ANTIDOTE
N-Acetylcysteine (NAC)
2 types:
1/POFluimucil for 24 hr.
2/IV Acetadote for 21hr .
🔹 Main Roles:
•Glutathione precursor
Restores hepatic glutathione stores
→
•Glutathione substitute
Directly binds the toxic metabolite (NAPQI)
→
•Enhances sulfation pathway
Facilitates non-toxic metabolism of APAP
→
•Antioxidant effect
Reduces oxidative stress, aids liver recovery
→
Time-Sensitive Efficacy
•Most effective when started within 8–10 hours
of ingestion
•Delayed therapy still helpful but less protective
against liver damage
18.
N-ACETYLCYSTEINE (NAC)
- OralNAC (Fluimucil) has unpleasant taste and smell prefer to be given in fruit juice
or by NG tube.
- IV NAC (Acetadote) indicated for :
1/ Interactable vomiting
2/ Hepatic Failure
3/ Pregnancy
IV NAC administered as 3% 30mg/ml solution in 5% dextrose ; this associated
some times with anaphylaxis Non Ige mediated - > stop NAC , Treat anaphylaxis ,
once patient is stable restarting NAC slowly
19.
N-ACETYLCYSTEINE AKA NAC
Dosage:
PONAC Fluimucil : 140 mg/kg loading, followed by 70 mg/kg q4h
IV NAC Acetadote : 150 mg/kg over 1 hr., followed by 50 mg/kg over 4 hr.,
followed by 100 mg/kg over 16 hr.
20.
TREATMENT: PROPHYLACTIC
By definitionthese patient has normal AST
APAP level known + within 24 hr. -> use the monogram to decide for NAC or not.
Any patient within possible/probable hepatotoxic range -> start NAC
AST and APAP should be followed to the end of interval , conditions:
1. AST normal ,APAP present (known or unknown time) -> continue NAC till non-detectable
APAP then stop .
2. AST elevating -> patient move to hepatic injury category
21.
TREATMENT: HEPATIC INJURY
Mostpatients' liver enzymes will peak 3 or 4 days after their ingestion
In this category of patients , you will find:
High AST at first , Then ALT , and lastly high INR
Any patient with this category should START NAC
If the LFTs falling you can discontinue NAC ( don’t rely on clinical findings) .
22.
TREATMENT: ACUTE LIVERFAILURE
King’s College Criteria : determine which patient is for liver transplant
1/Academia pH <7.3 after adequate fluid ( Alone indicate transplant)
2/Coagulopathy INR >6
3/Renal dysfunction Creatinine >3.4mg/dl
4/Grade 3 or 4 Hepatic encephalopathy
Lactic Acid >3mmol/L with criteria above means death if liver transplant not done.
23.
TREATMENT: REPEATED SUPRATHERAPEUTIC
INGESTION
Usuallydue to Unintentional overdose through ingestion of multiple medications containing the drug
Or simply person assume it to be save at any dose
Ingestion of high dose daily leads to hepatic injury
The monogram not beneficial in this case .
Conditions:
Asymptomatic:
AST normal , APAP < 10 microgram/ml -> no therapy needed
AST normal , APAP high -> start NAC till “non-detectable”
AST high -> treat as hepatic injury category
Symptomatic , ( RUQ pain , vomiting , jaundice ,etc. ..) treat Empirically with NAC don’t wait for labs.
24.
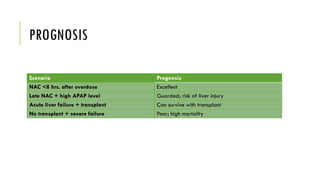
PROGNOSIS
Scenario Prognosis
NAC <8hrs. after overdose Excellent
Late NAC + high APAP level Guarded; risk of liver injury
Acute liver failure + transplant Can survive with transplant
No transplant + severe failure Poor; high mortality
25.
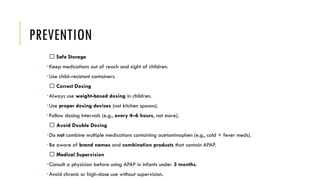
PREVENTION
✅ Safe Storage
•Keepmedications out of reach and sight of children.
•Use child-resistant containers.
✅ Correct Dosing
•Always use weight-based dosing in children.
•Use proper dosing devices (not kitchen spoons).
•Follow dosing intervals (e.g., every 4–6 hours, not more).
✅ Avoid Double Dosing
•Do not combine multiple medications containing acetaminophen (e.g., cold + fever meds).
•Be aware of brand names and combination products that contain APAP.
✅ Medical Supervision
•Consult a physician before using APAP in infants under 3 months.
•Avoid chronic or high-dose use without supervision.
26.
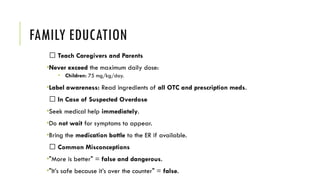
FAMILY EDUCATION
🧠 TeachCaregivers and Parents
•Never exceed the maximum daily dose:
• Children: 75 mg/kg/day.
•Label awareness: Read ingredients of all OTC and prescription meds.
🆘 In Case of Suspected Overdose
•Seek medical help immediately.
•Do not wait for symptoms to appear.
•Bring the medication bottle to the ER if available.
💬 Common Misconceptions
•"More is better" = false and dangerous.
•"It’s safe because it’s over the counter" = false.
27.
REFERENCES
1. Nelson Textbookof Pediatrics 21st
ed. – chapter 77 - p.
2430
2. Illustrated Reviews: Pharmacology 7th
ed. – chapter 44 -
p.1664
3. The essentials of forensic medicine and toxicology 33rd
ed. - chapter 37 – p. 658
4. MOH Pocket Manual in Emergency Medicine – Chapter 4
– p.100
Editor's Notes
#2 Drug names are :
1/ chemical name
2/ Generic name assigned by official bodies (like WHO or USAN Council)
3/ Brand name
---------------------
Formulations : IV, IM , PO , SUPPOSITORY
STRENGHTS : Pediatric formulations: usually 120 mg, 160 mg per 5 mL syrup
Adult tablets/capsules: 325 mg, 500 mg, sometimes 650 mg
Suppositories: 125 mg, 250 mg, 500 mg
IV dose: varies but commonly 1 gram per dose
COMBINATIONS: PARACETAMOL WITH ( CAFFIENE , CODIENE , IBUPROFEN, ETC…)
#4 Analgesic:
Acts in the CNS, inhibiting central COX → ↓ prostaglandins (PGE2) → ↓ pain perception.
Antipyretic:
Acts on the hypothalamus, inhibiting prostaglandins → resets thermostat → ↓ fever via vasodilation and sweating.
Reye syndrome : Viral infection + aspirin -> Mitochondrial damage (brain & liver ) -> no beta oxidation -> Fatty liver disease + brain swelling
High ammonia , hypoglycemia ,Lactic acidosis , brain swelling
#6 Oral APAP undergo first pass metabolism in the liver 95% , only <5 % is work and after 30 to 60 min
IV APAP bypass this part and firstly and large amount done its job , but in the end the came to liver by same percentage
#11 - Signs of liver failure/cirrhosis : vomiting,
jaundice, hepatic pain, bleeding, hypoglycemia,
confusion, coma, metabolic acidosis and coarse
flapping tremor of hands (asterixis).
-There may be
cardiac arrhythmias, hemorrhagic pancreatitis,
disseminated intravascular coagulation,
#12 2* to make sure that all particles of APAP had been absorbed
#13 Before 4 hr. not useful because the amount ingested not absorbed completely.
After 24 hr. nomogram is not useful -> Rely on Clinical Manifestations & Labs
#15 7y.o most probably unintentional poisoning
Step1 : 5000mg÷25kg=200mg/kg so we need measure APAP , do we need to plot? Yes bcz its more than 150
Step 2 : APAP = 180 now -> more than 150 in nomogram start NAC
#16 Activated Charcoal 1-2 hr. of ingestion , it binds APAP in stomach i.e. before absorption. (adsorption)
#19 Fluimucil is a mucolytic also . Used in respiratory diseases to treat respiratory secretions.
#20 Normal AST, So we manage them to prevent hepatic injury
#21 AST first because It found in the mitochondria & cytoplasm , so with necrosis the mitochondria died and release AST before ALT that found in cytoplasm .
AST have shorter half life ,While ALT have longer
INR describing PT increase if the liver loss its ability to form clotting factors 2,7,9,10.
Discontinue therapy in the clinically well patient remains controversial
#22 Here we move from the previous hepatic injury to more sever hepatic failure , which will indicate the transplantation if met the criteria .