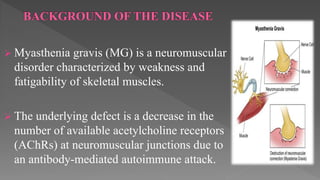
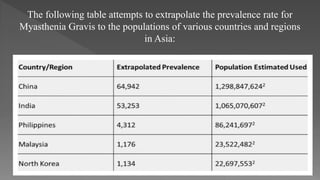
Myasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by muscle weakness and fatigability due to the decrease in acetylcholine receptors at neuromuscular junctions. Symptoms commonly include drooping eyelids, double vision, and difficulty with speech and swallowing, with various treatments available to manage symptoms but no known cure. The condition is more prevalent in women and typically affects individuals over 40 years of age, especially in regions like China and India.