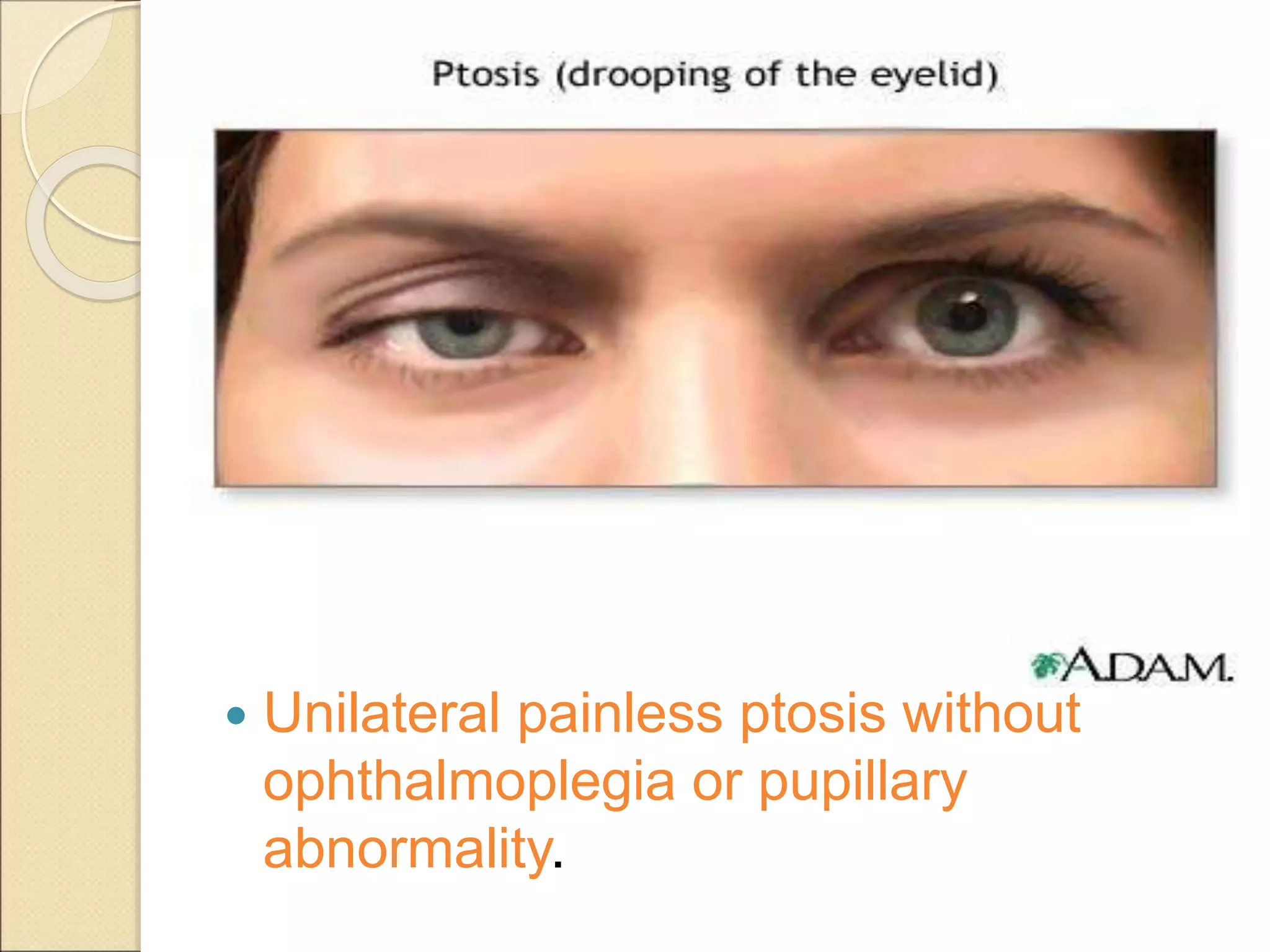
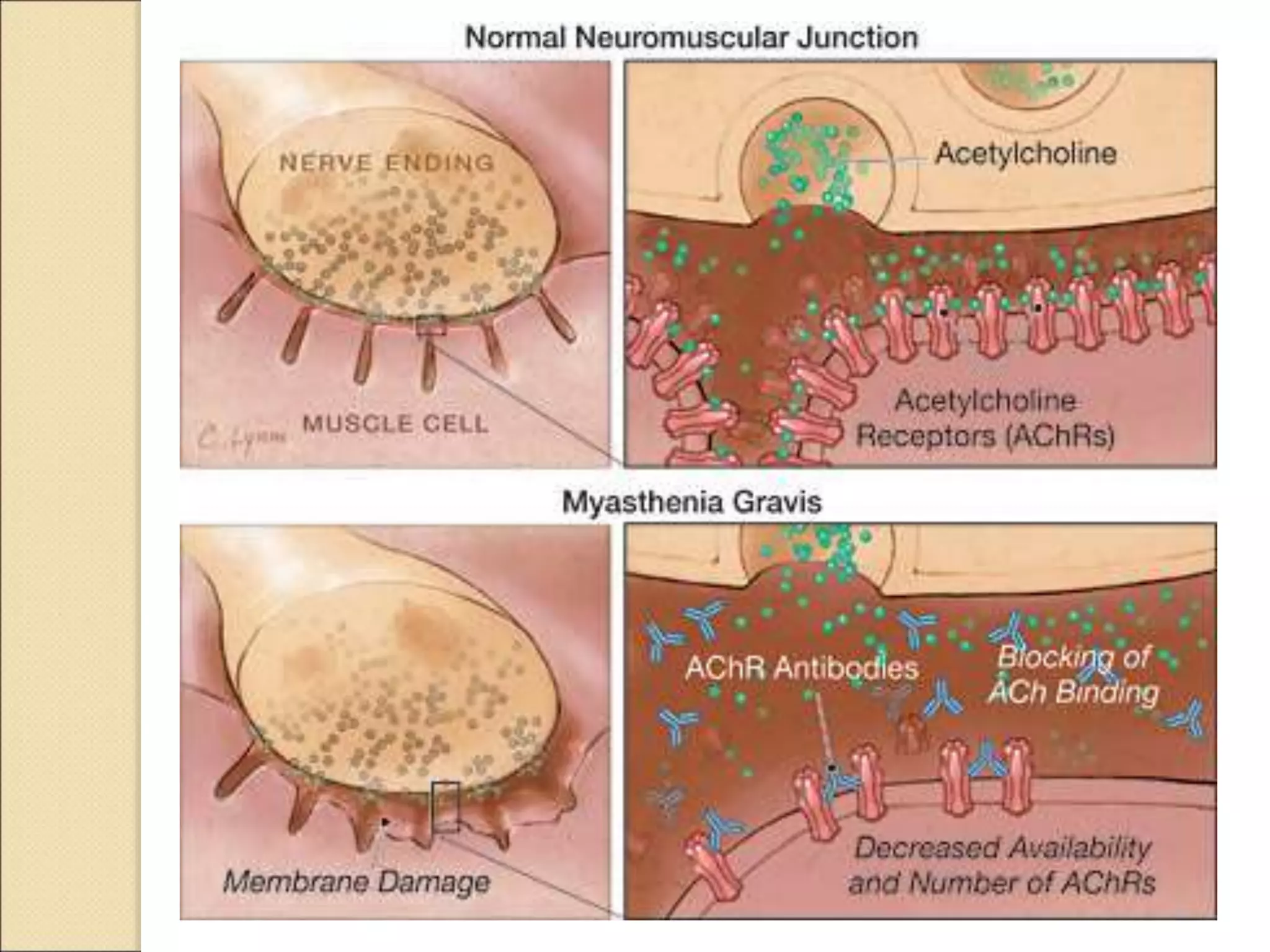
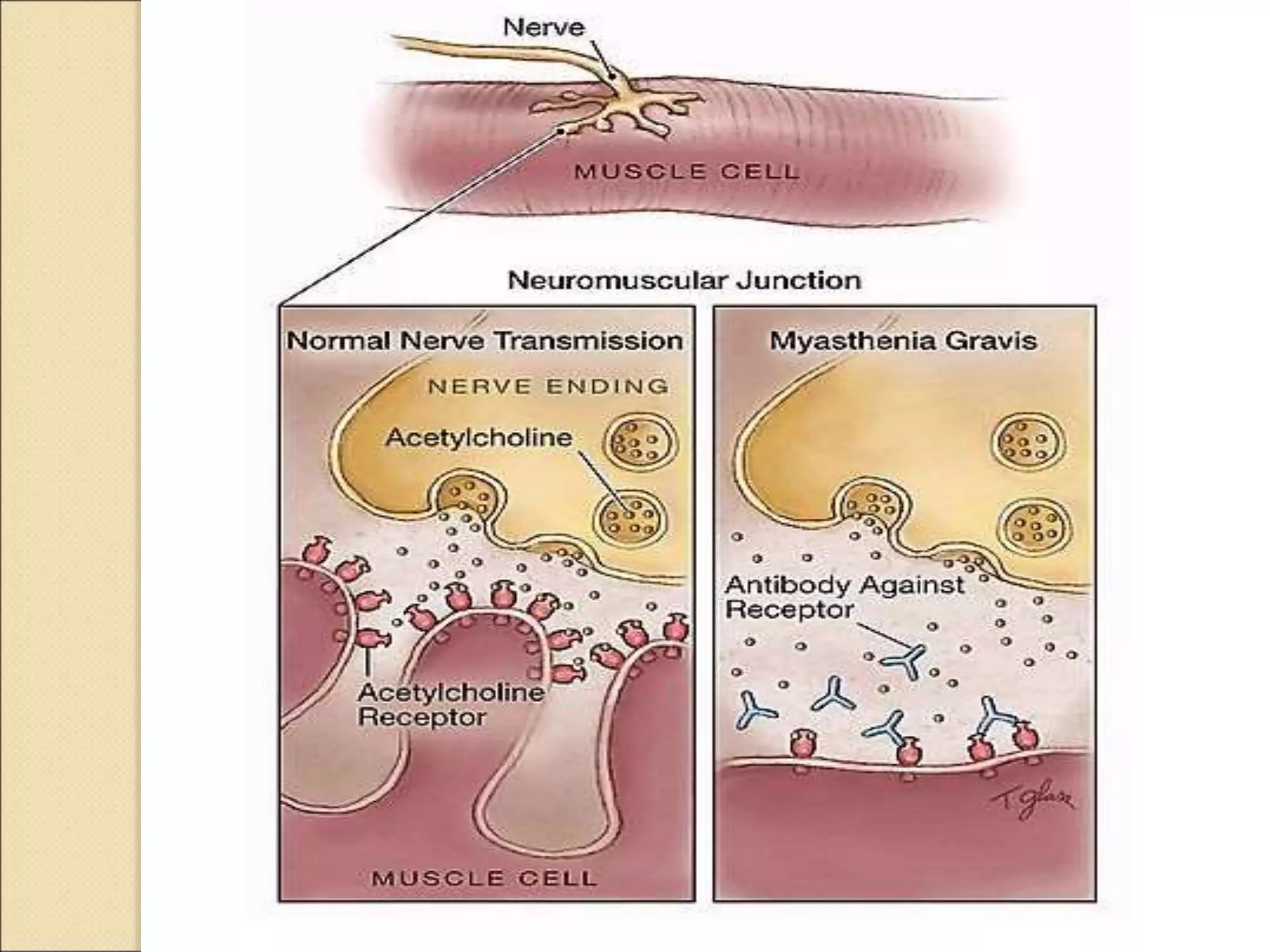
Myasthenia Gravis is a neuromuscular disorder characterized by fluctuating weakness that worsens with activity and improves with rest. It results from antibodies blocking or lessening the effects of acetylcholine at the neuromuscular junction. Symptoms often begin with weakness of the eye muscles or face. While treatments can help control symptoms, there is currently no cure. Management involves anticholinesterase medications, immunosuppressants, plasmapheresis, thymectomy, and ventilatory support during myasthenic crises.





















































































![INSULIN AND OTHER ANTIDIABETEC DRUGS [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/insulinandotherantidiabetecdrugsautosavedautosaved-220731124033-32b4f1bb-thumbnail.jpg?width=640&height=640&fit=bounds)











![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













