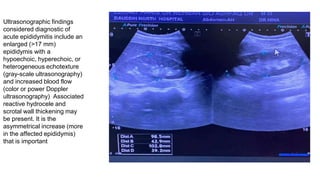
Samina Hussain presented a case of a 33-year-old male who presented to the emergency room with complaints of testicular swelling for 3 days and fever for 3 days. On examination, he was found to have erythematous swelling of the left testis with tenderness and a positive Prehn's sign. Ultrasound showed an enlarged epididymis. He was diagnosed with acute epididymitis and started on IV hydration, antibiotics, and analgesics. Mumps and resulting orchitis were discussed as a possible cause.










































![Mumps[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mumps1-200930140514-thumbnail.jpg?width=640&height=640&fit=bounds)




























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









