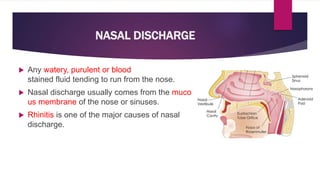
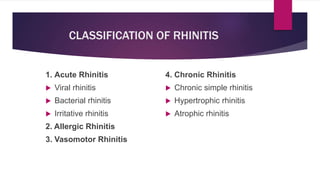
This document discusses nasal discharge and its various causes. It begins by classifying rhinitis into acute and chronic forms. Acute rhinitis can be viral, bacterial, or irritative. Chronic rhinitis includes chronic simple rhinitis, hypertrophic rhinitis, and atrophic rhinitis. Allergic rhinitis and vasomotor rhinitis are also discussed. The document provides details on symptoms, treatments, and complications for each type of rhinitis. It also covers other conditions like sinusitis, CSF rhinorrhea, and their clinical presentations.