Download to read offline

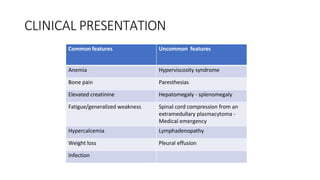
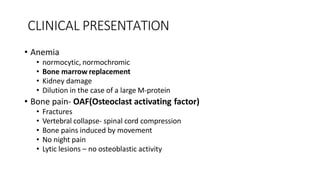
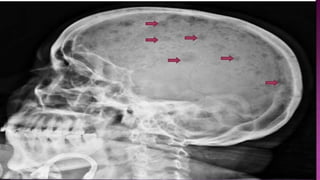
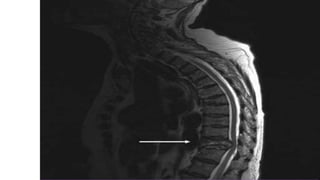
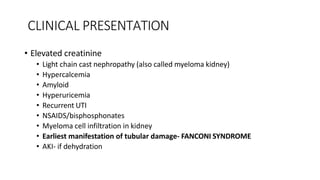
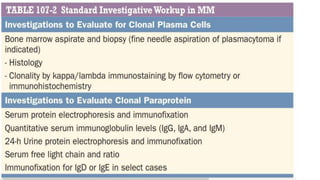
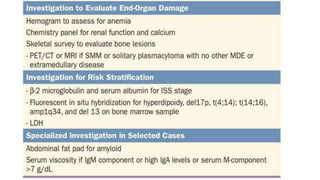
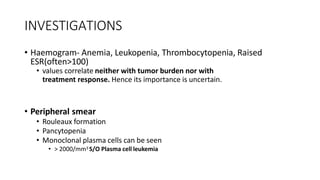
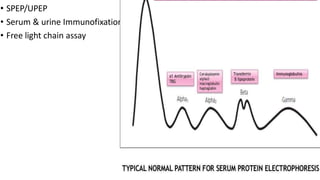
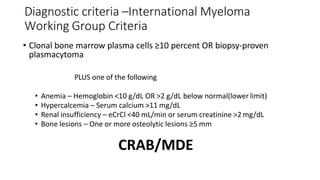
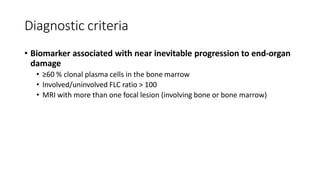

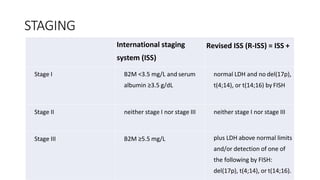
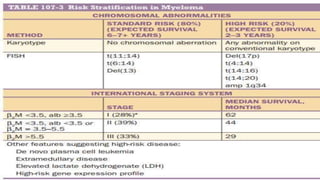
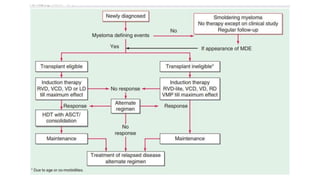
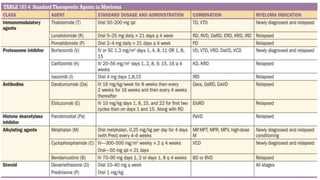



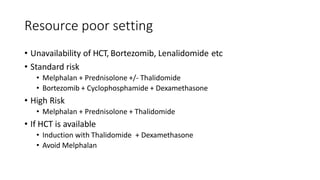

Multiple myeloma is a neoplastic proliferation of plasma cells that produce monoclonal immunoglobulins. It commonly presents with anemia, bone pain, elevated creatinine, and fatigue. Diagnosis requires clonal bone marrow plasma cells ≥10% plus biomarkers of end organ damage like hypercalcemia, renal insufficiency, or bone lesions. Treatment involves managing complications, chemotherapy like bortezomib/lenalidomide with dexamethasone, and sometimes stem cell transplant. Prognosis depends on staging systems like ISS which incorporate serum albumin and beta-2 microglobulin levels.
















![Multiple myeloma[1]](https://cdn.slidesharecdn.com/ss_thumbnails/multiplemyeloma1-190414034945-thumbnail.jpg?width=640&height=640&fit=bounds)






































































