Downloaded 366 times


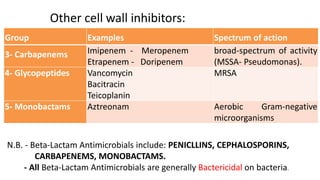
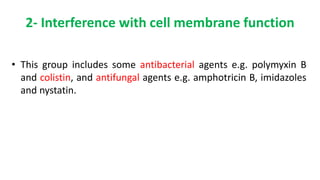
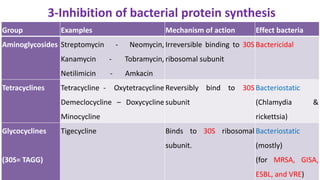
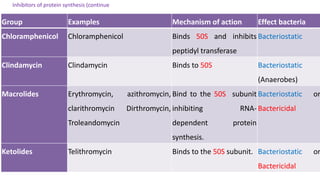

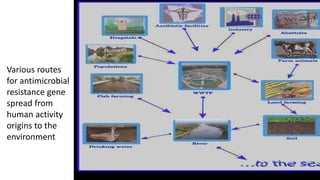

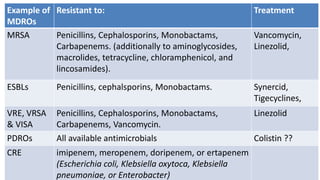
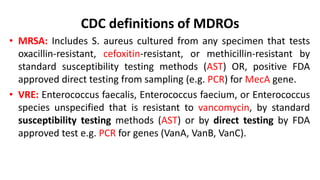
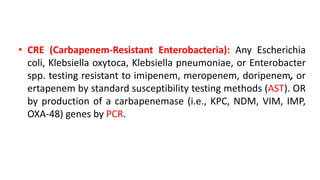
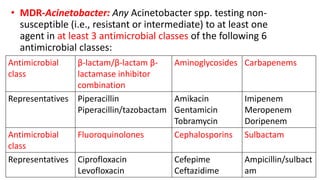
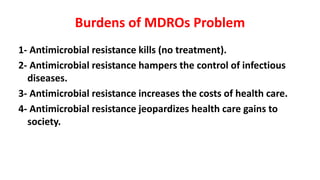
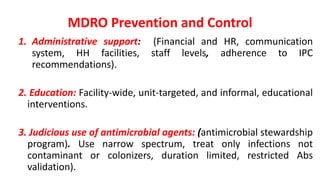




The document discusses multi-drug resistant organisms (MDROs), detailing the genetic factors, classifications, mechanisms of action, and resistance mechanisms of various antimicrobial agents. It explains how bacteria can develop resistance through natural and acquired methods, highlighting the roles of mobile genetic elements in the spread of antimicrobial resistance. Examples of resistant bacteria and their susceptibility patterns are provided, emphasizing the public health threat posed by MDROs.























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















