Terms
Antibiotic: Chemical producedby a microorganism that kills or
inhibits the growth of another microorganism
Antimicrobial agent: Chemical that kills or inhibits the growth
of microorganisms
3.
MIC = Minimalinhibitory concentration.
Lowest concentration of antimicrobial that inhibits growth of
bacteria.
Commonly used in clinical lab
MBC = Minimal bactericidal concentration.
Concentration of an antimicrobial that kills bacteria.
Used clinically only in special circumstances
4.
• Susceptible: theantibiotic is effective against the bacteria
• Resistant:the bacteria can grow even if the drug is present
• Breakpoint = The MIC that is used to designate between
susceptible and resistant.
– Arbitrarily set by a committee
•
5.
• Antimicrobial Resistance
•Relative or complete lack of effect of antimicrobial against a
previously susceptible microbe
• Increase in MIC
6.
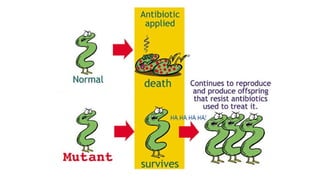
Antibiotic resistance isa type of drug resistance where a
microorganism is able to survive exposure to an antibiotic.
Resistant organism: One that will not be inhibited or killed by
an antibacterial agent at concentrations of the drug achievable
in the body after normal dosage.
Factors contributing forresistance
Misuse of antibiotics
Use of antibiotics with no clinical indication (e.g, for viral infections)
Use of broad spectrum antibiotics when not indicated
Inappropriate choice of empiric antibiotics
Overuse of antibiotics
Addition of antibiotic to the feed of livestock
Failure to follow infection control practices
9.
Why resistance isimportant
• Resistant organisms lead to treatment failure
• Increased mortality
• Resistant bacteria may spread in community
• Low level resistance can go undetected
• Added burden on healthcare costs
• Threatens to return to pre-antibiotic era
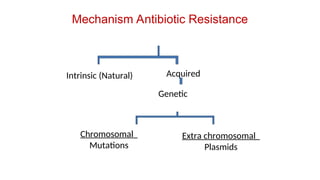
Antibiotic resistance inbacteria
Two types:
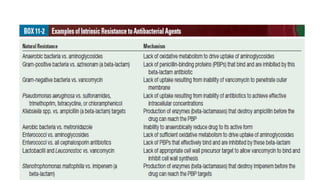
Intrinsic:
Naturally occuring trait
Species or genus specific
Acquired:
Acquired resistance implies that a susceptible organism has developed resistance to
an agent to which it was previously susceptible
can occur in two general ways: by mutation (s) in the existing DNA of the organims
or by acquisition of new DNA.
Present in only certain strains of a species or of a genus
16.
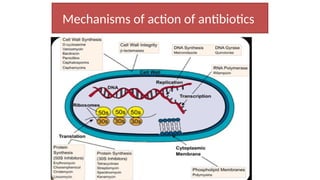
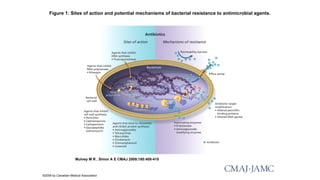
Antibiotics Resistance
• Thefour main mechanisms of antibiotic resistance are
• (1) enzymatic degradation of the drug
• (2) modification of the drug's target
• (3) reduced permeability of the drug
• (4) active export of the drug.
• Most drug resistance is the result of a genetic change in the
organism, caused either by a chromosomal mutation or the
acquisition of a plasmid or transposon.
17.
Genetic Basis ofResistance
• Chromosomal mutations
– A single chromosomal mutation may result in the synthesis of an
altered protein
– change the target of the drug so that the drug does not bind or
– change the membrane so that the drug does not penetrate well into
the cell.
18.
Genetic Basis ofResistance
Chromosomal mutations
Chromosomal mutations occur at a low frequency (perhaps 1 in 10
million organisms), and often affect only one drug or one family of
drugs.
streptomycin resistance via alteration in a ribosomal protein
the single aminoacid change in the enzyme dihydtropteroate synthetase
resulting in a lowered affinity for sulfonamides
A series of mutations, for example, changes in penicillin binding proteins
(PBPs) in penicillin resistant pneumococci
19.
Genetics of Resistance
Resistance by acquisition of new DNA
– By Transformation
– Conjugation
– Transduction
Nature of elements involved in transferring DNA:
Plasmids: plasmid mediated resistance much more efficient than the
resistance ass. with chromosomal mutation
Transposons
20.
Plasmids
• Extra chromosomalgenetic elements can replicate
independently and freely in cytoplasm.
• Plasmids which carry genes resistant ( r-genes) are called R-
plasmids.
• These r-genes can be readily transferred from one R-plasmid to
another plasmid or to chromosome.
• Many of the drug resistance encountered in clinical practice is
plasmid mediated
21.
Plasmids
• Resistance plasmids(R plasmids, R factors) usually carry two
sets of genes.
– One set encodes the enzymes that degrade or modify drugs
– the other encodes the proteins that mediate conjugation
22.
Mechanisms of ResistanceGene Transfer
• Transfer of r-genes from one bacterium to
another
Conjugation
Transduction
Transformation
• Transfer of r-genes between plasmids within
the bacterium
By transposons
By Integrons
23.
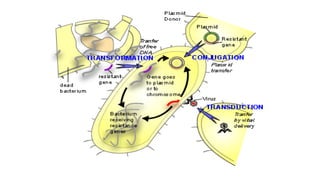
Transfer of r-genesfrom one bacterium to another
Conjugation : Main mechanism for spread of resistance
The conjugative plasmids make a connecting tube
between the 2 bacteria through which plasmid itself
can pass.
Transduction : Less common method
The plasmid DNA enclosed in a bacteriophage is
transferred to another bacterium of same species.
Seen in Staphylococci , Streptococci
Transformation : least clinical problem.
Free DNA is picked up from the environment (i.e..
From a cell belonging to closely related or same strain.
25.
Mechanisms of ResistanceGene Transfer
Transposons
Transposons are small pieces of DNA
that move from one site on the
bacterial chromosome to another or
from the bacterial chromosome to
plasmid DNA.
Transposons often carry drug
resistance genes.
Many R plasmids carry one or more
transposons.
26.
The donorplasmid containing the transposons, co-integrate
with acceptor plasmid
They can replicate during cointegration
Both plasmids then separate and each contains the r-gene
carrying the transposon.
Mechanisms of Resistance Gene Transfer
Transposons
27.
Mechanisms of ResistanceGene Transfer
Integrons
Integron is a large mobile DNA can spread multidrug
resistance
Each Integron is packed with multiple gene casettes, each
consisting of a resistance gene attached to a small recognition
site.
These genes encode several bacterial functions including
resistance and virulence.
They cannot promote self transfer
28.
Resistance mechanisms
Enzymatic inactivation
Microbescan also express drug resistance genes that code
for enzymes that covalently
modify the antimicrobial drug, thereby reducing its antimicrobial
activity
Mutations, plasmid and/or transposones
Beta-lactam, Aminoglycoside, Chloramphenicol, Macrolids
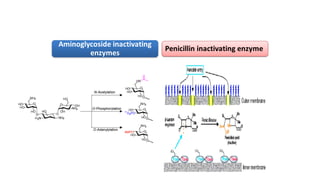
Resistance mechanisms
• Enzymaticinactivation
• Aminoglycoside
– ACT N-acetyltransferase, which acetylates an NH2 group of the
aminoglycoside molecule
– APH O-phosphotransferase, which phosphorylates an OH group of the
aminoglycoside molecule
– ANT O-adenyltransferase, which adenylates an OH group of the
aminoglycoside molecule
• Chloramphenicol
– Acetyltransferases, which acetylate and thereby inactivate
chloramphenicol
32.
Resistance mechanisms
Decreased Permeability
Decreaseduptake(impermeability) and increased efflux of drug from
the microbial cell
Decreased uptake of antimicrobial drugs and/or use of transmembrane efflux pumps prevents the
concentration of antimicrobial agent from increasing to toxic levels within the microbial cell
(↓uptake↓conc↓effect).
33.
Resistance mechanisms
Outermembrane may provide an extra barrier
against drug uptake (especially hydrophobic drugs)
in Gram negative bacteria, which is not present in
Gram positive bacteria
This is one explanation why Gram negative bacteria
are less susceptible than Gram positive bacteria to
many antibiotics, including beta-lactams and
macrolids
34.
Resistance mechanisms
Efflux Pumps
Activationof efflux pumps by mutation or plasmids
Quinolones, macrolids, tetracyclins
1. The major facilitator subfamily (MFS),
2. The resistance nodulation cell division subfamily (RND),
Pseudomonas aeruginosa (MexAB)
3. The small multidrug regulator subfamily (SMR),
4. The adenosine triphosphate (ATP)-binding cassette (ABC) family
5. The multidrug and toxic effects (MATE) family.
35.
Resistance mechanisms
Target Alteration
Expressionof resistance genes that code for an altered
version of the substrate to which the antimicrobial agent
binds
GENE mutation → translated to altered
protein( substrate) → low binding affinity→ reduced
antibacterial activity → resistance developed
36.
Resistance to β-lactams:
Resistance due to β -lactamases: most prevalent
Alteration in the pre-existing penicillin binding
proteins (PBPs)
Acquisition of a novel PBP insensitive to beta β –
lactams: e.g, methicillin resistance in
Staphylococcus aureus (MRSA)
Changes in the outer membrane proteins of Gram
negative organisms that prevent these compounds
from reaching their targets
37.
Resistance to β-lactams
• β –lactamases
– TEM, SHV, KPC, VIM…
– Effect different betalactams
• Methicillin resistance
– If bacteria resistance to methicillin, bacteria accepted resistant against
penicillins and cephalosporins
– By mecA ans MecCgene PBP2a
– PBP2a shows low affinity to betalactams
– mecA gene PBP2a low affinity to betalactams cell wall synthesis continues
38.
Aminoglycoside Resistance:
– Resistanceto aminoglycosides is mediated by three main
mechanisms:
– modification of the drug by
• phosphorylating, adenylylating, and acetylating
enzymes,
– Mutations in the genes encoding one of the 30S ribosomal
proteins,
– Reduced permeability
39.
Tetracycline resistance
• Mostcommon antibiotic resistance encountered in
nature
• Mechanisms:
– Altered permeability due to chromosomal mutations
– Active efflux or Ribosomal protection (by production of a
protein) resulting from acquisition of exogenous DNA
40.
Macrolids
Macrolide, Lincosamide andStreptogramin resistance:
Resistance to erythromycins is primarily caused by a plasmid-
encoded enzyme that
methylates the 23S ribosomal RNA, thereby blocking binding of the drug.
– Intrinsic resistance is due to low permeability of outermembrane
protein
– Drug inactivation and active efflux may also occur
41.
Quinolone resistance
Resistanceto quinolones is primarily caused
by mutations in the gene encoding the
bacterial DNA gyrase
Decreased permeability
Efflux pumps
42.
Glycopeptide resistance
Alterationof target
Resistance to vancomycin is caused by a change in the D-ala-D-
ala part of the peptide in peptidoglycan to D-ala-D-lactate,
Vancomycin binds to d-Ala–d-Lac with markedly lower affinity
than it does to the normal dipeptide product
43.
• Van genesmainly cause glycopeptide resistance
• Van A-G
• Van A is the most common, confers resistance to vancomycin
and teicoplanin
• VanC is chromosomal in E. casseliflavus and E.gallinorum