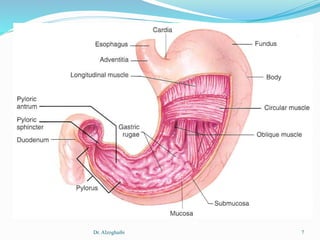
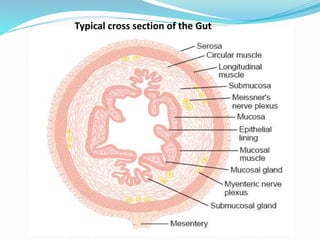
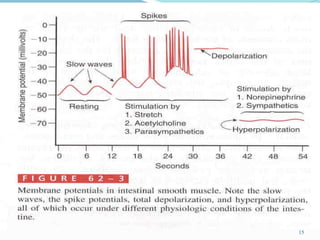
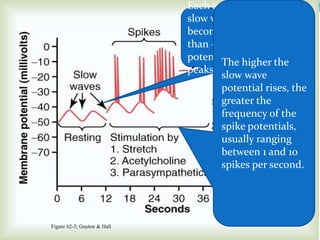
This document discusses gastrointestinal physiology, specifically focusing on the musculature of the digestive tract. It describes the main muscle layers - longitudinal and circular muscles - and how their contractions function to move food through the tract. It also discusses the electrical activity of the muscles, including slow waves and spike potentials generated by interstitial cells of Cajal that control the rhythm of movements. Contractions can be either phasic with relaxation, seen in most of the tract, or tonic without relaxation, as in sphincters.