
This document describes Monteggia fractures and dislocations. It begins by defining the injury as described by Monteggia in 1814. It then discusses Bado's classification system from 1967 which categorized Monteggia injuries into four main types based on the location of the ulna fracture and direction of radial head dislocation. The document provides details on the mechanisms of injury, signs, treatment approaches including closed reduction and casting or surgical intervention depending on the fracture type and stability of the reduction. Complications are also outlined.
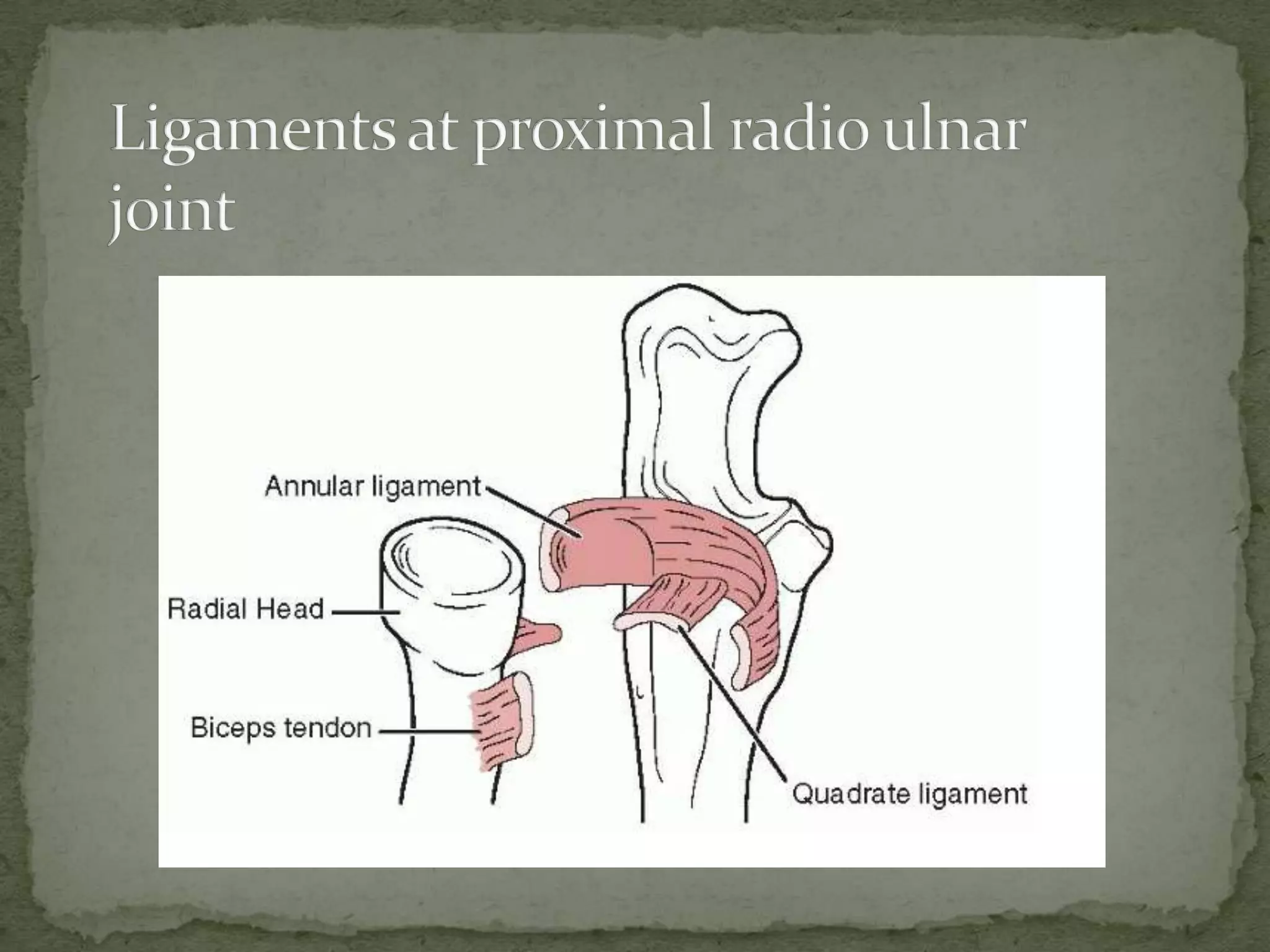
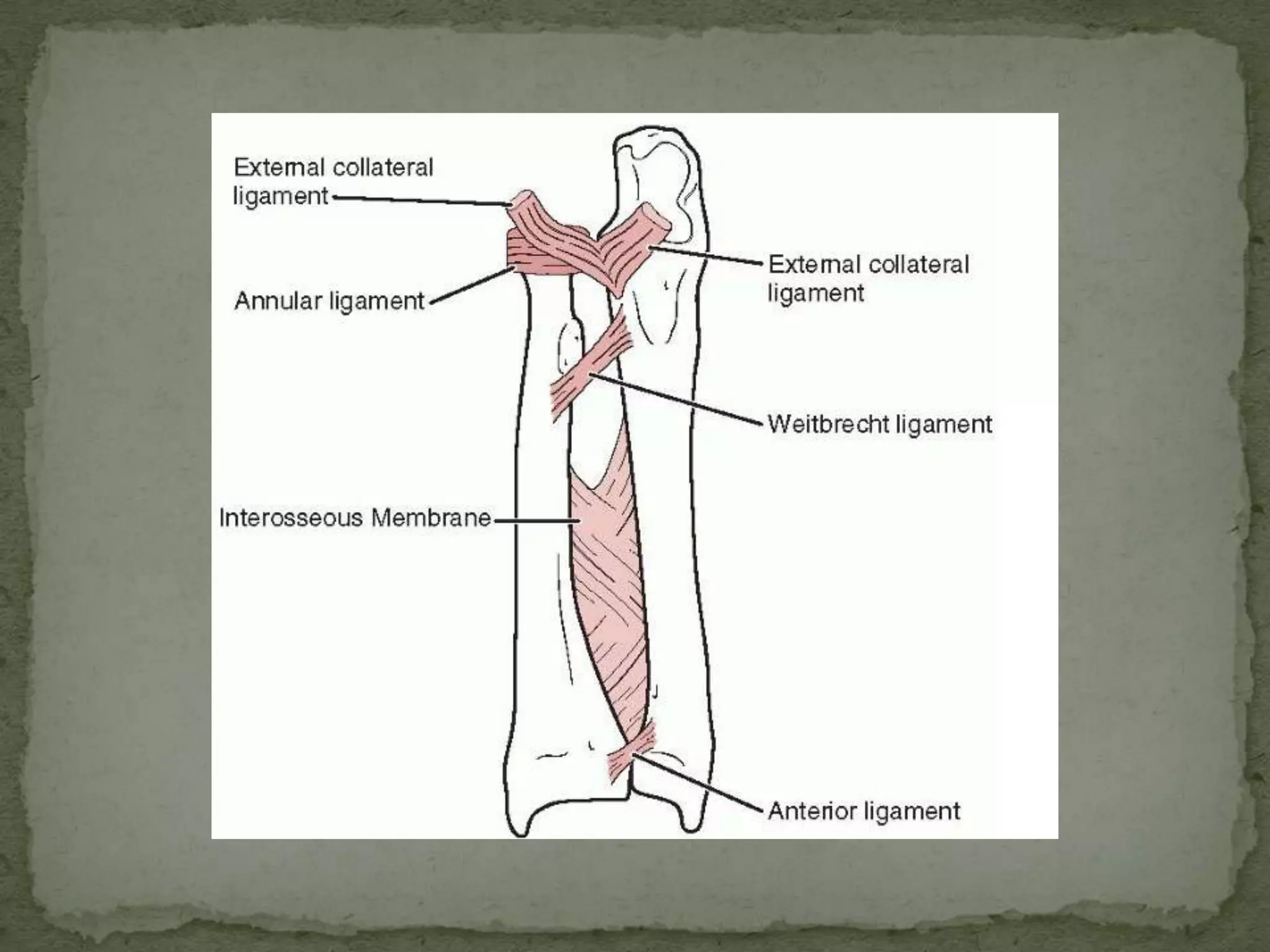
Introduced by Monteggia and classified by Bado in 1967, focusing on ulna fractures and radial dislocations, primarily in children aged 4-10.
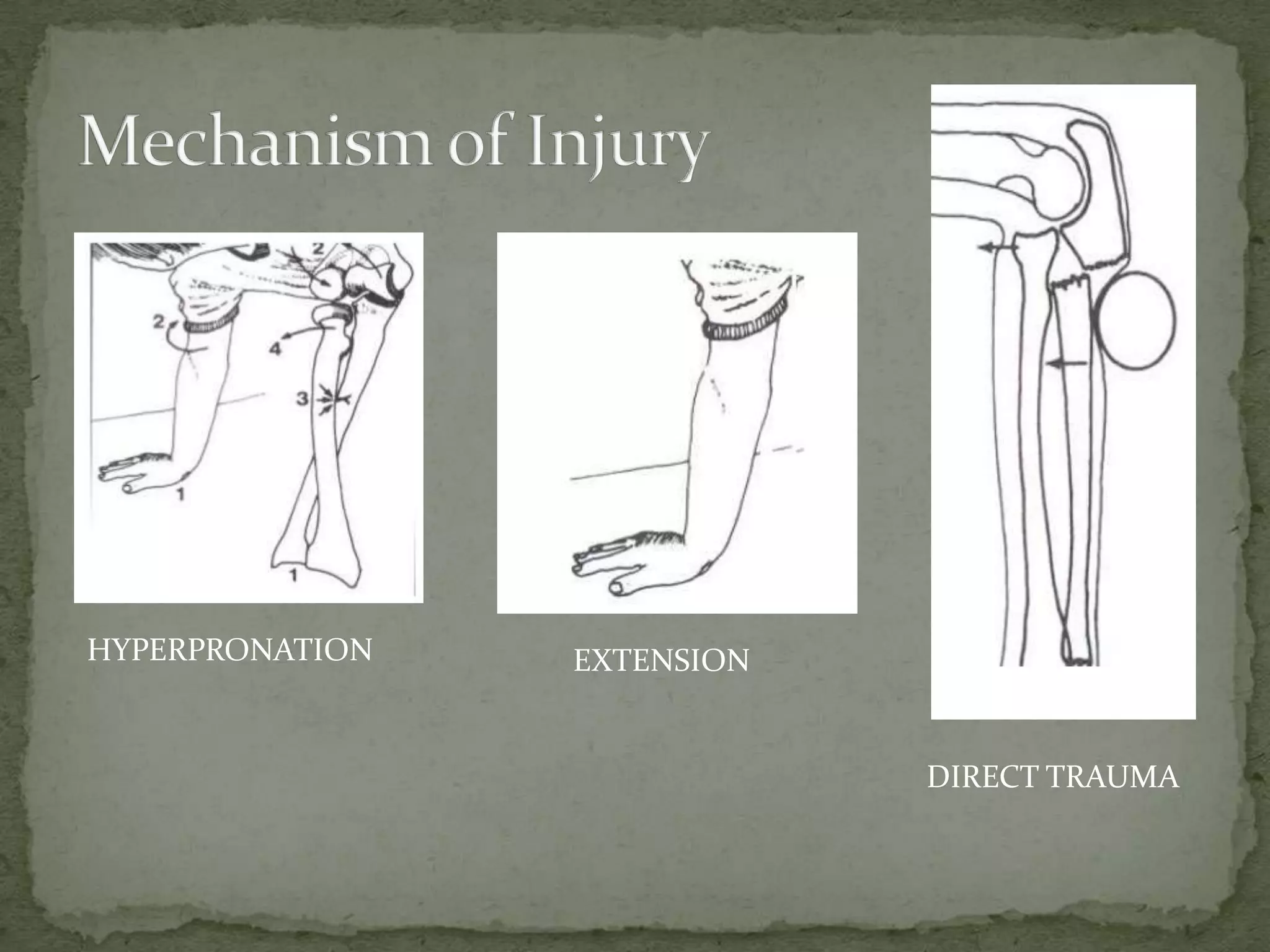
Describes injury mechanisms such as hyperpronation, extension, and direct trauma leading to elbow fractures.
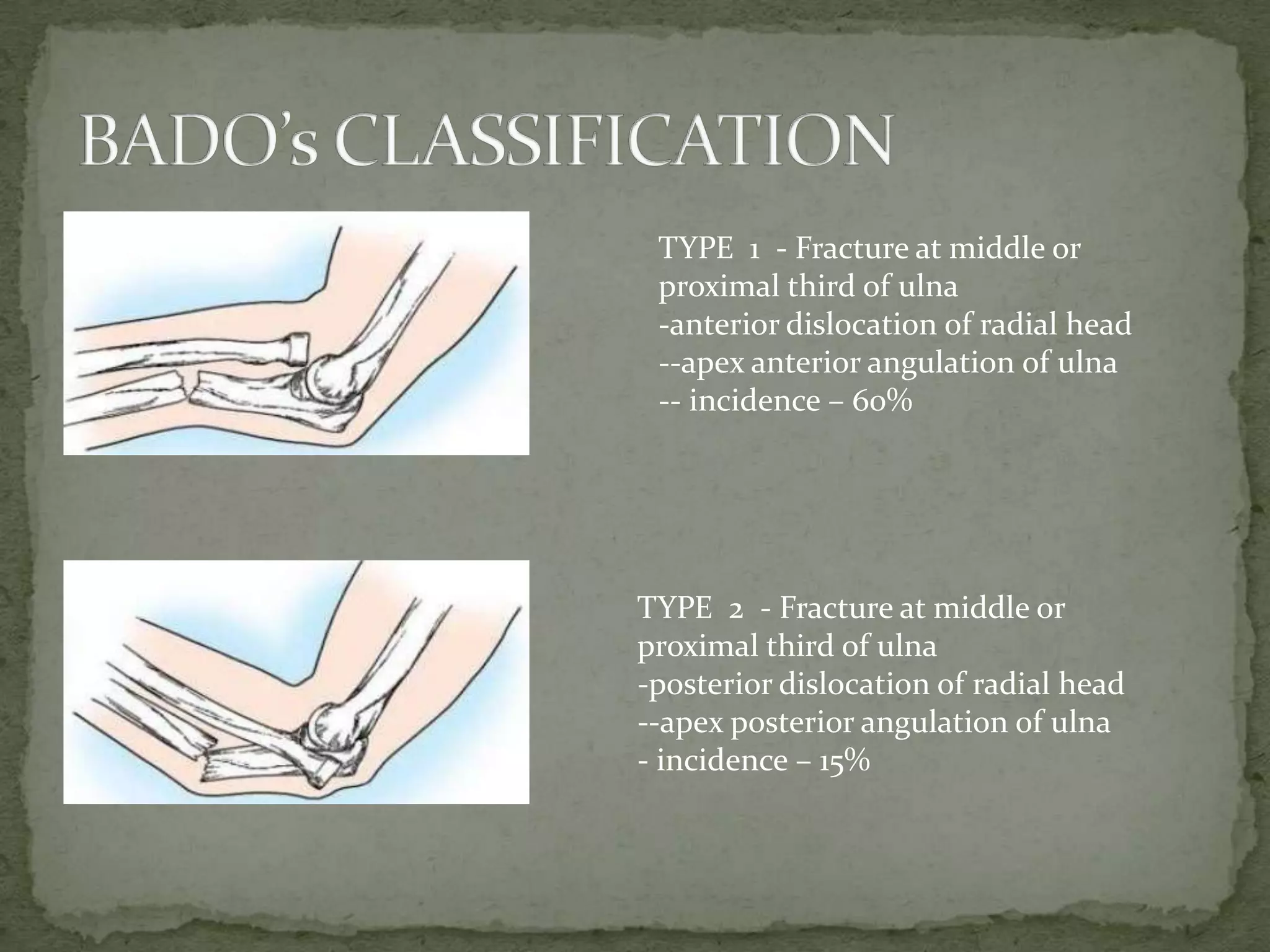
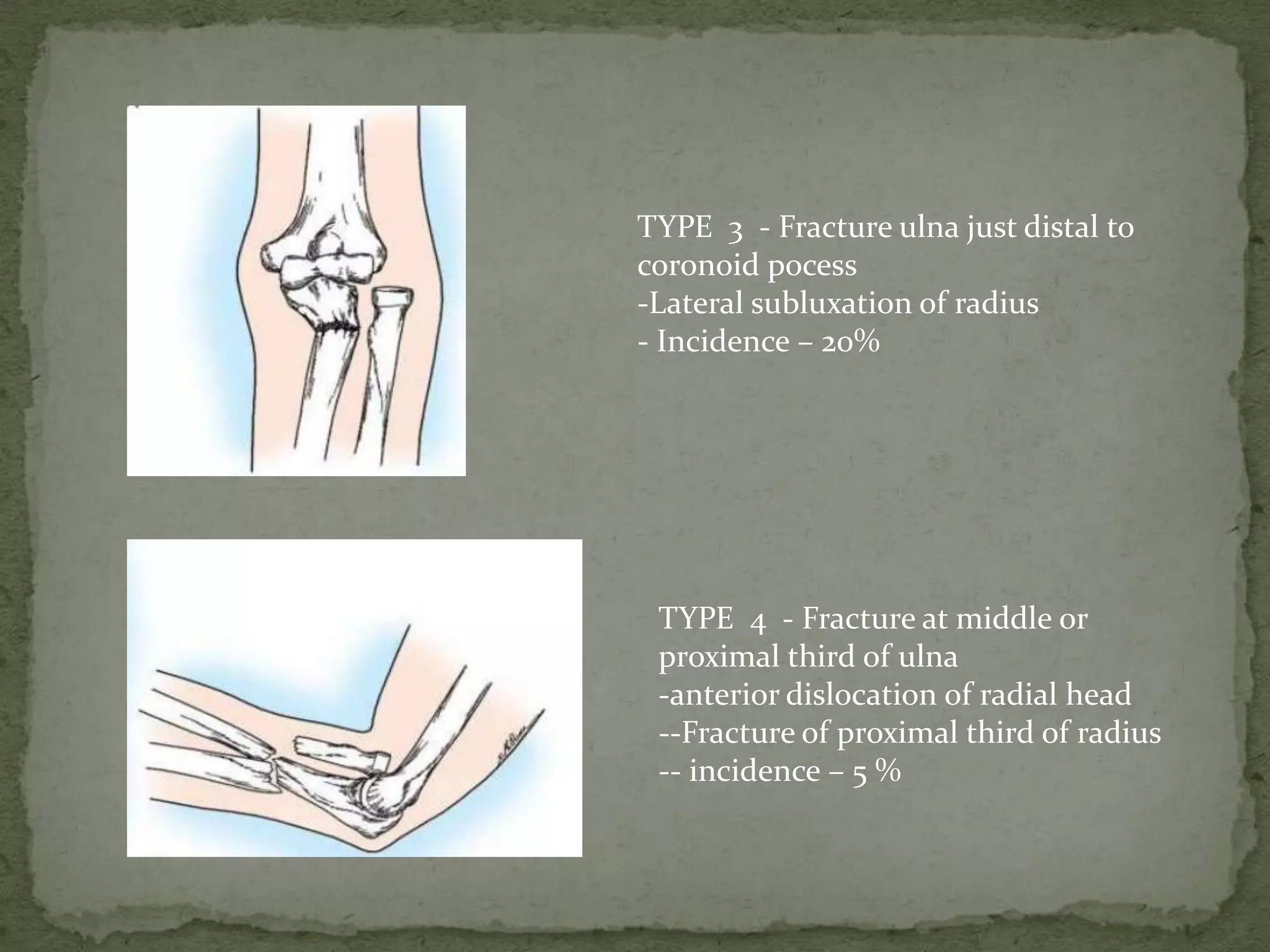
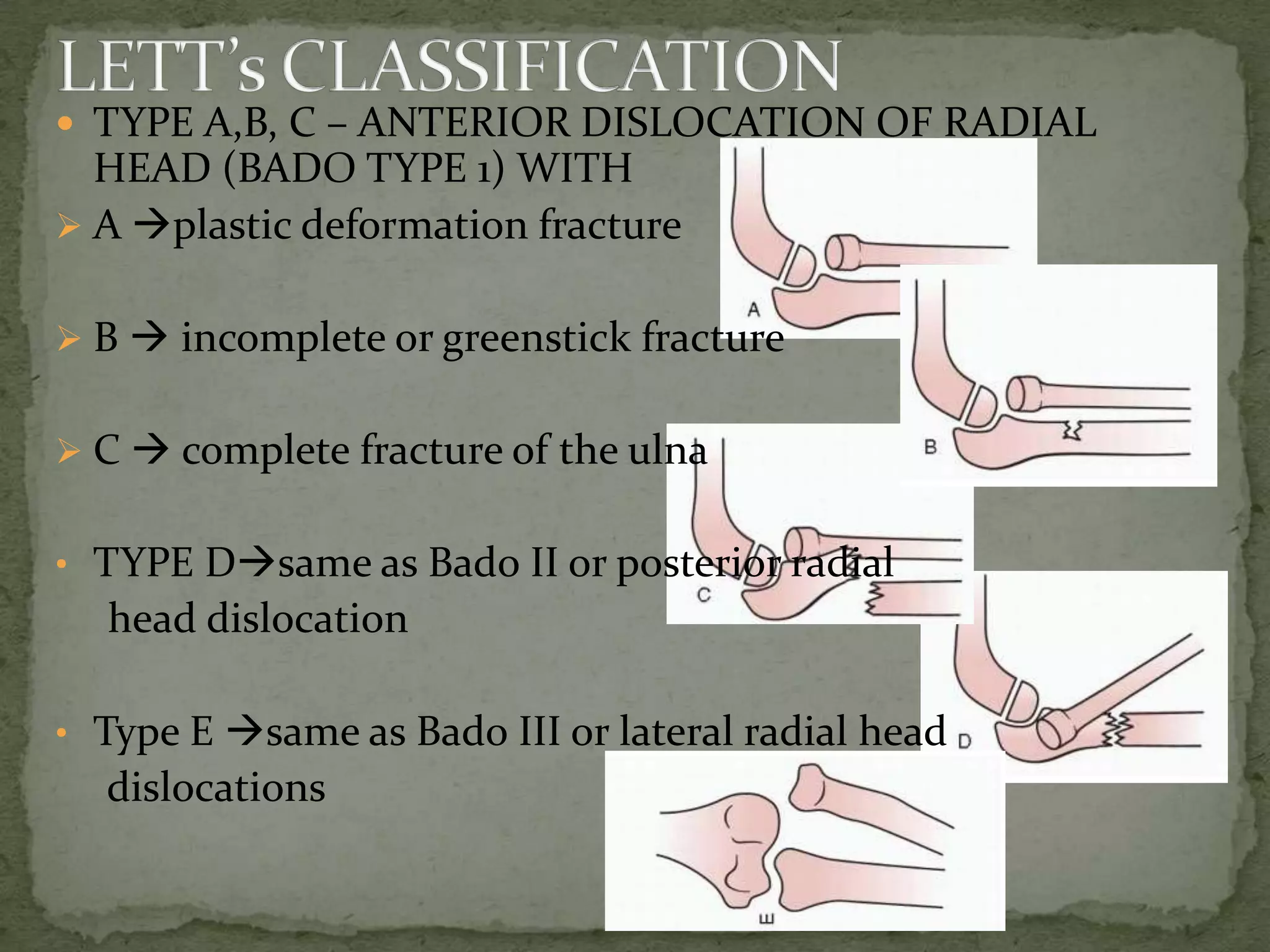
Breakdown of Bado's types of fractures: Types 1-4 with respective incidence rates and characteristics like dislocations of the radial head.
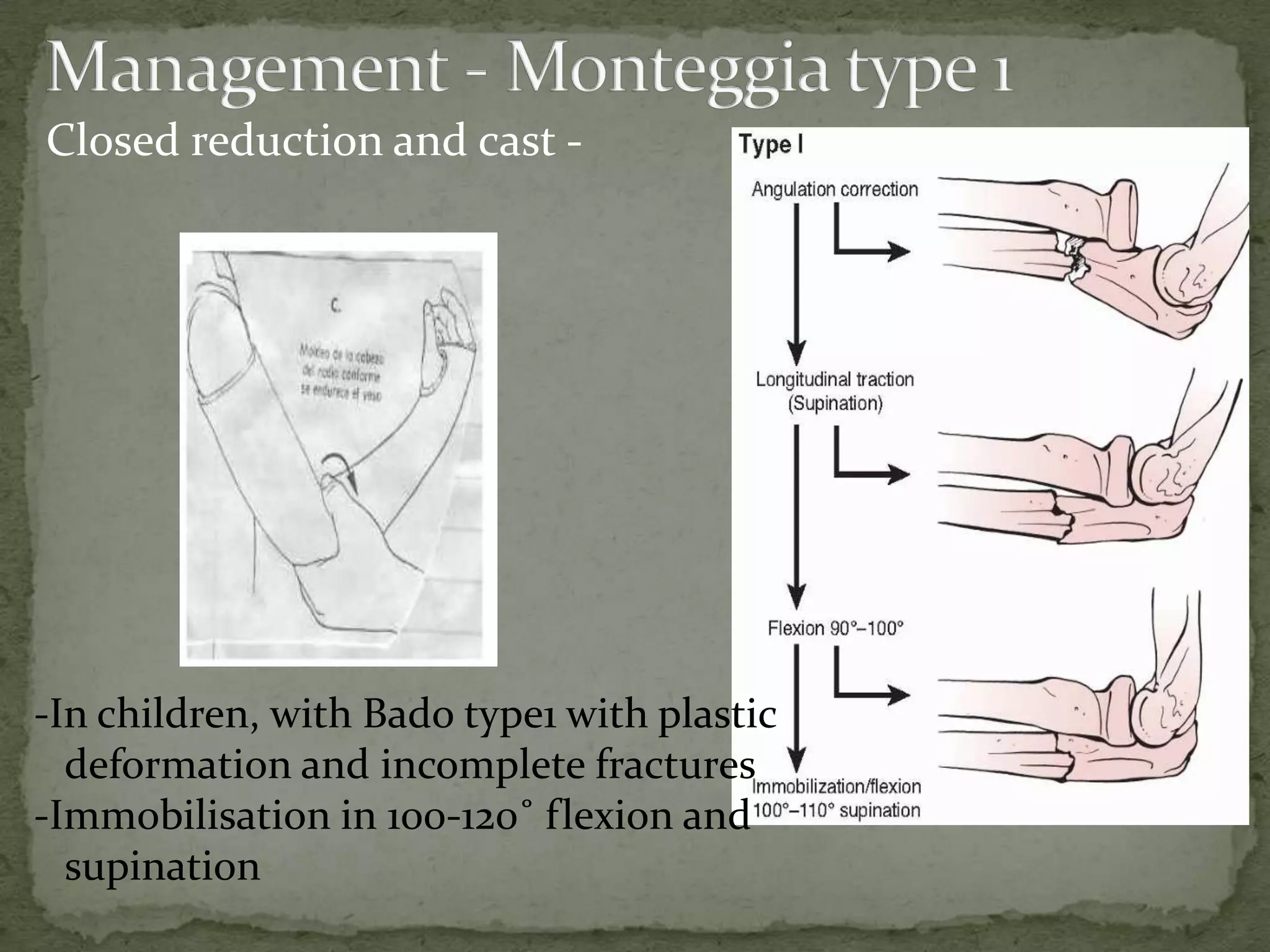
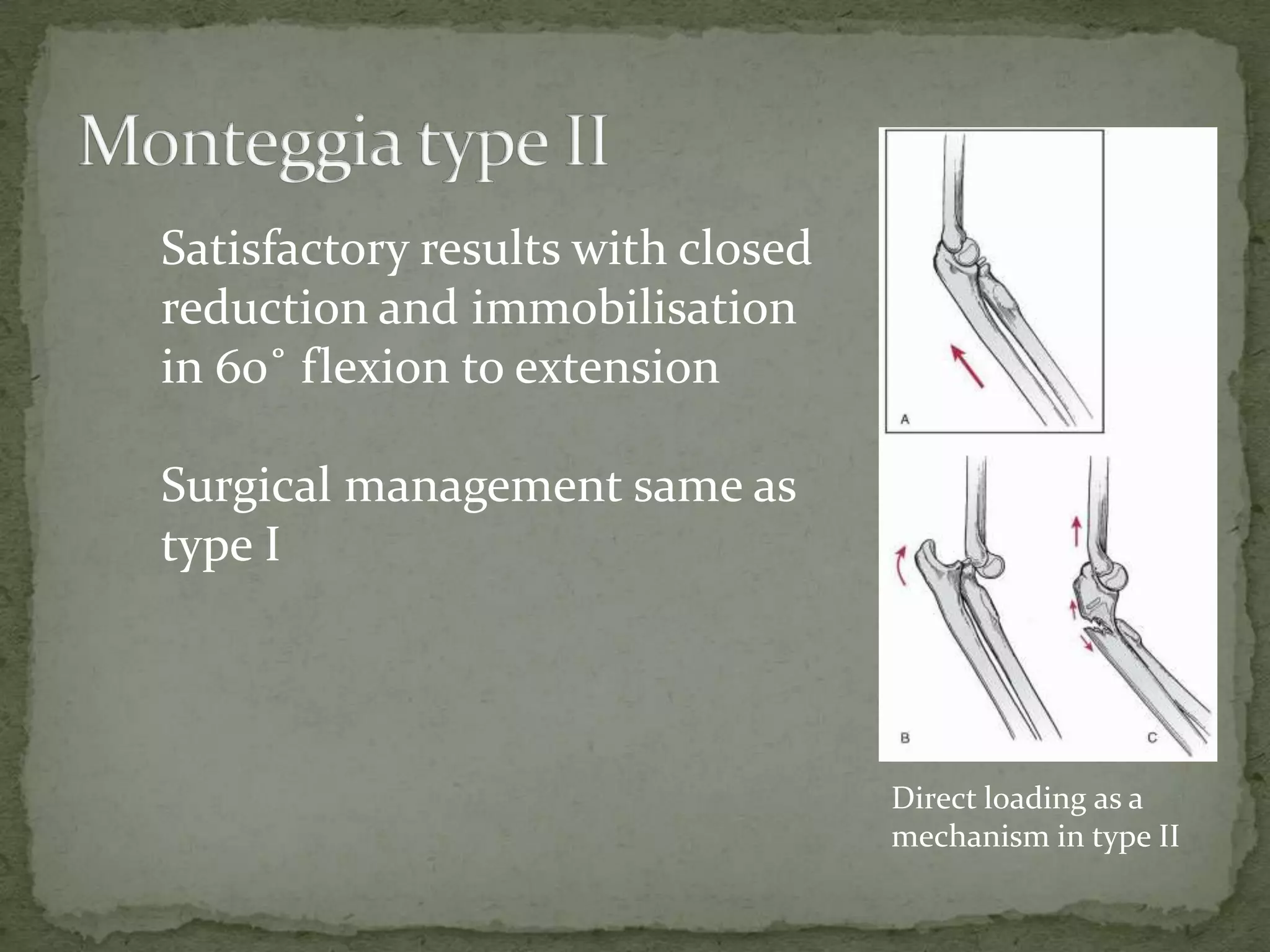
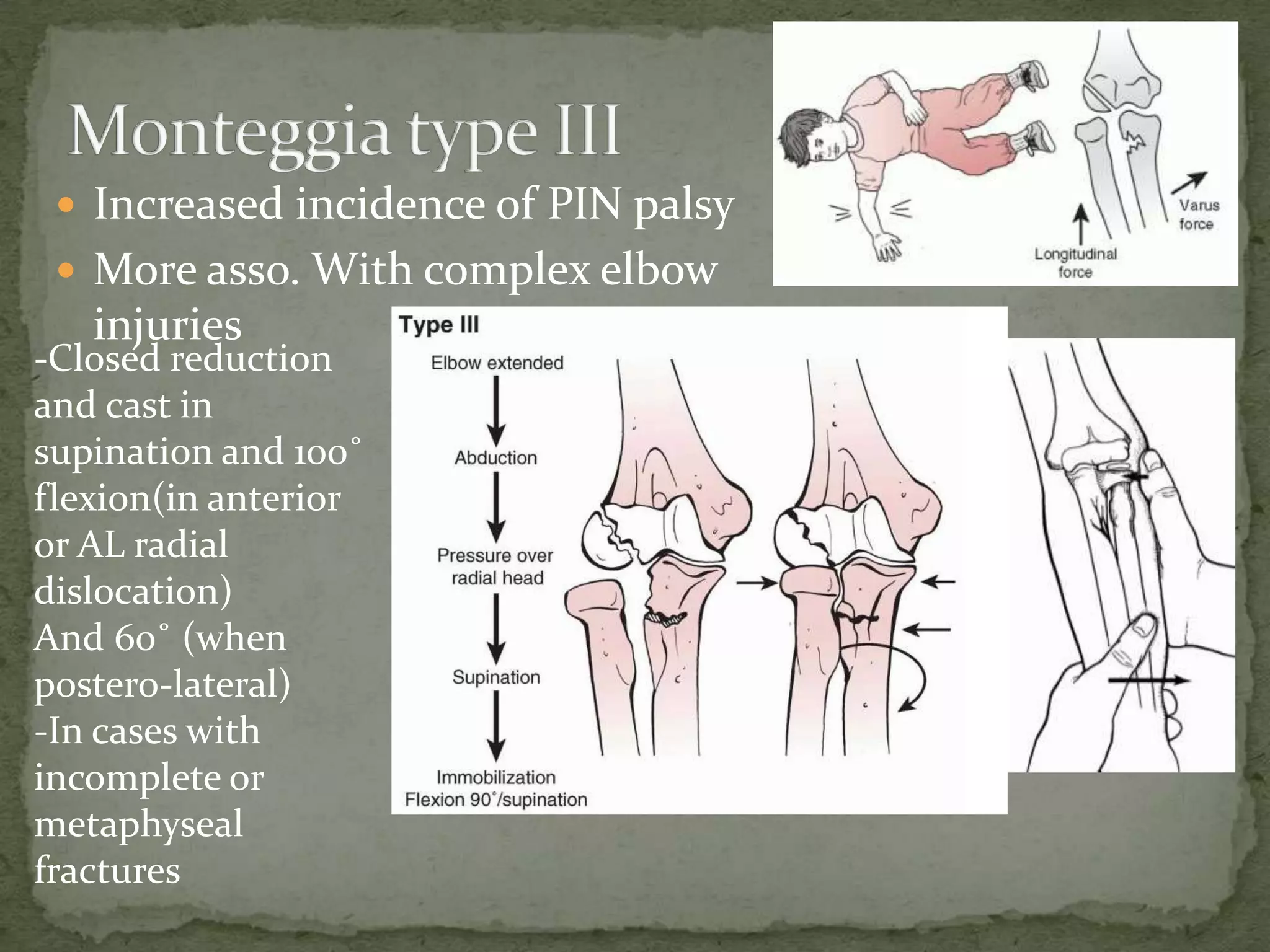
Closed reduction strategies for Bado types, including casting and surgical options for fractures, highlighting rehabilitation considerations.
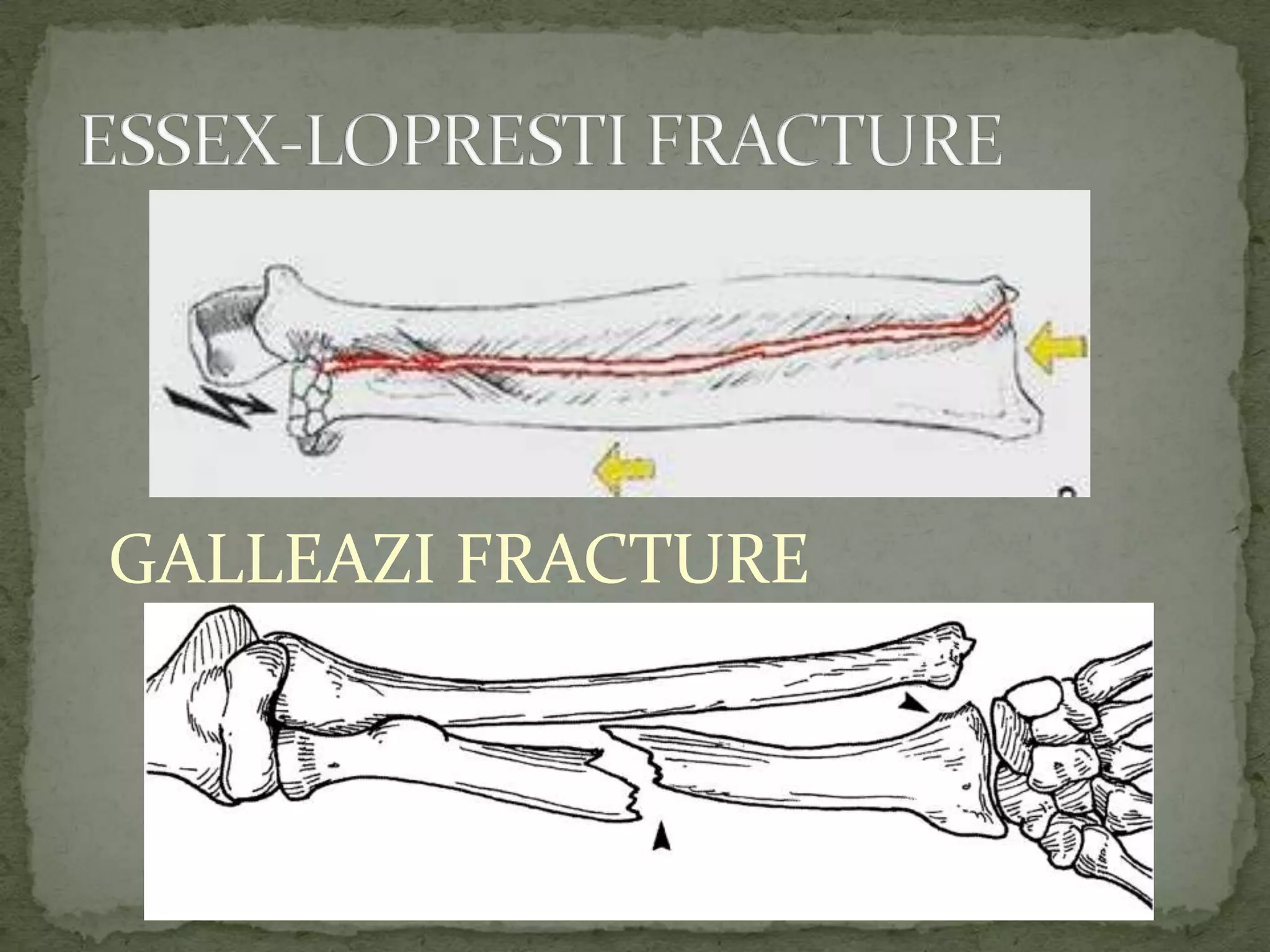
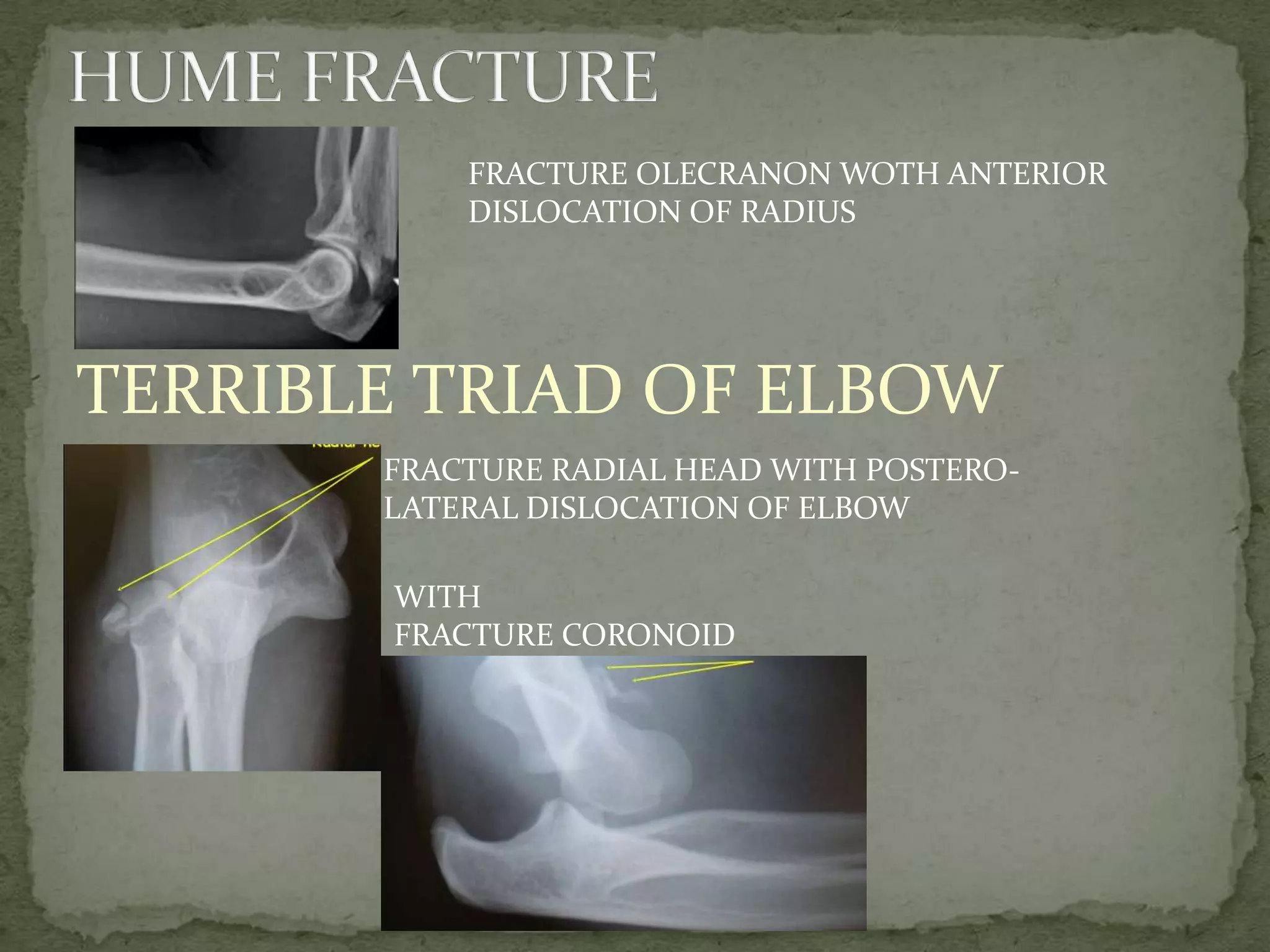
Discusses complications like PIN palsy, criteria for surgical intervention, and various reconstruction techniques for radial and ulnar repairs.Identification of complex injury types including Gallazi fractures and the terrible triad of elbow, emphasizing fracture patterns.