Downloaded 405 times
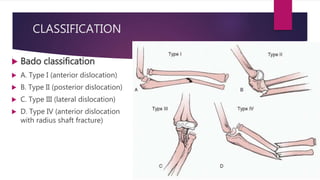
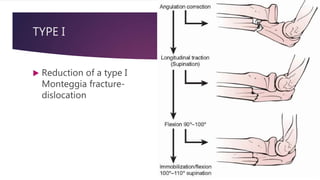


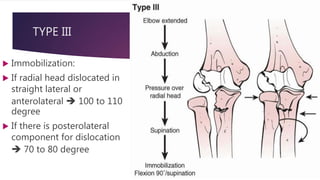
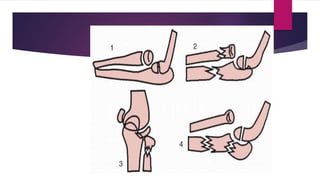
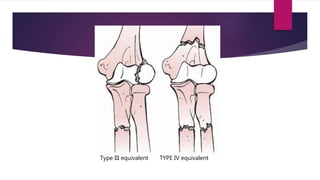

The document summarizes the Monteggia fracture-dislocation classification system in children. It describes the four types of Monteggia injuries (Types I-IV) based on the location of the ulna fracture and direction of radial head dislocation. For each type, it provides details on injury mechanism, clinical findings, treatment approach including closed or open reduction, and immobilization methods. It also discusses associated injuries and Monteggia equivalent lesions that present similarly to the four main types.









































































