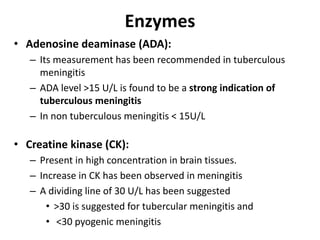
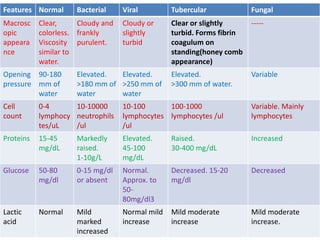
The document is a detailed presentation on meningitis, outlining its causes, types, and diagnostic methods, particularly focused on cerebrospinal fluid (CSF) analysis. It includes information on sample collection, normal CSF findings, and specific tests for distinguishing between bacterial, viral, and tubercular meningitis. Key indicators such as glucose levels, protein content, and various enzymes are discussed to aid diagnosis and assessment of severity.