Downloaded 2,870 times
![ Hb, Hematocrit
RBC count
MCV (Hct x 10 / RBC x 106) [ 90±8 fl ]
MCH (Hb x 10 / RBC x 106) [ 30 ± 3 pg ]
MCHC (MCH/MCV) [ 33 ± 2 % ]
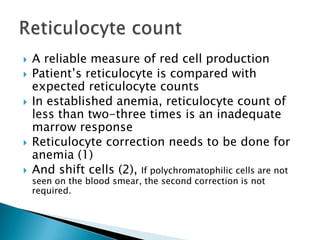
Reticulocyte count
Indices vary with age, gender and pregnancy
WBC count including differential count, neutrophil
segment count
Platelet count](https://image.slidesharecdn.com/approachtoanemia-121124124558-phpapp01/85/Approach-to-Anemia-11-320.jpg)
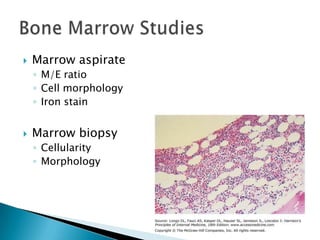
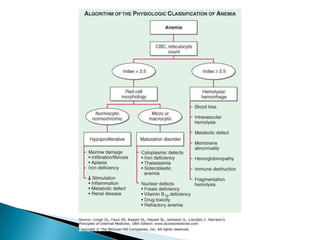
![ 43yrs / F, k/c/o Beta Thal Carrier
Generalised weakness x 7 days
Hb – 6.4g% (17/6)
7.0/26.4% on admission, 7 days later after
starting Mumfer
Tot RBC: 4.42 x 106 cells/mm3
MCV – 60 fl [78-98]
MCH – 16pg [27-32]
MCHC 27% [31-34]
TLC: 8000cells/cumm, N46 L44 M7 E2.1 B0.1
Plt: 289,000/cumm](https://image.slidesharecdn.com/approachtoanemia-121124124558-phpapp01/85/Approach-to-Anemia-37-320.jpg)



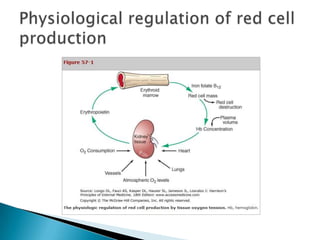
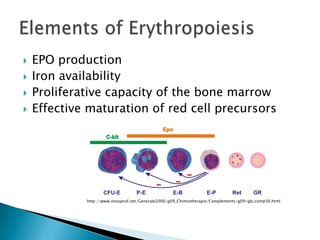
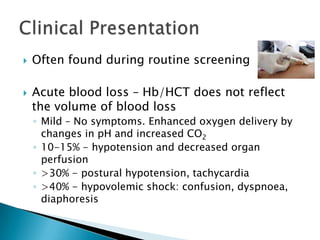
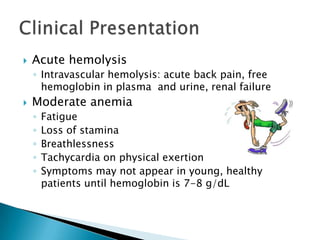
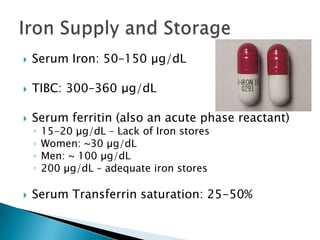
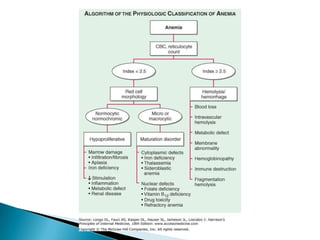
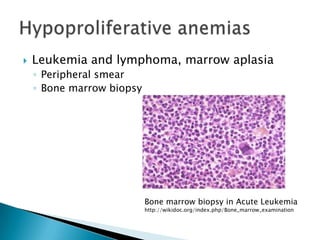
The document discusses anemia, defining it as a hemoglobin level below 130g/L for men and 120g/L for women. Anemia is initially classified based on erythropoiesis, which involves EPO production, iron availability, bone marrow proliferative capacity, and red blood cell maturation. Causes of anemia include blood loss, hemolysis, bone marrow diseases, and deficiencies. Evaluation involves history, exam, blood tests of cell counts and indices, smear examination, iron studies, and bone marrow analysis. Treatment depends on the underlying cause.



































































