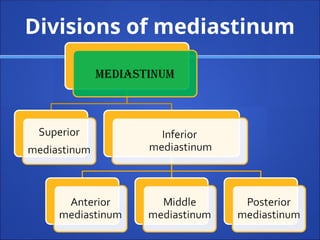
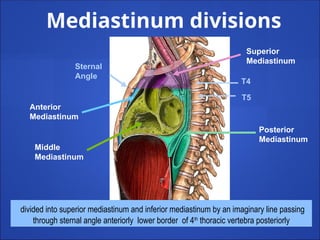
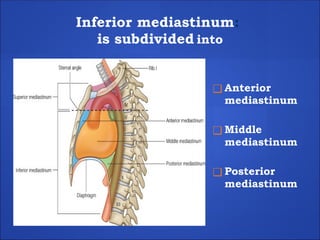
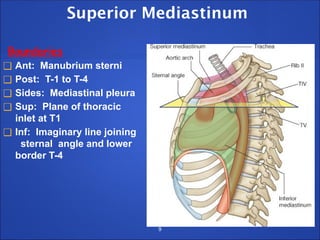
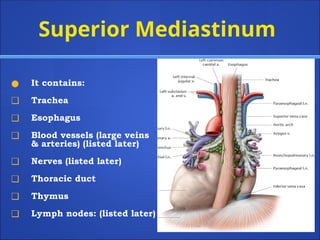
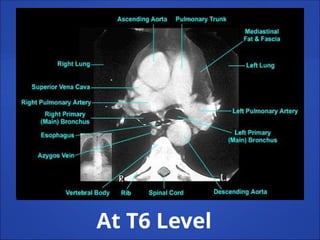
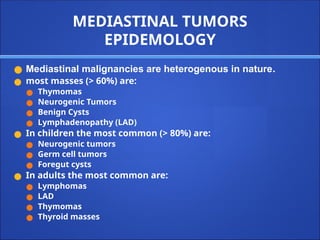
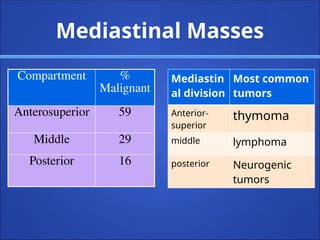
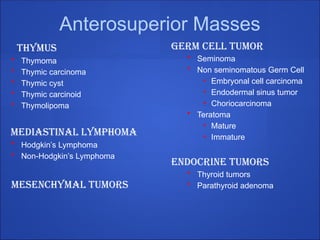
The document provides an extensive overview of the mediastinum, detailing its boundaries, divisions, and contents, including the superior, anterior, middle, and posterior mediastina. It discusses major structures present in each region, common mediastinal tumors, their epidemiology, and clinical presentations. The document also covers diagnostic imaging and the significance of mediastinal masses in relation to anatomical structures and malignancies.














































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





