Downloaded 342 times

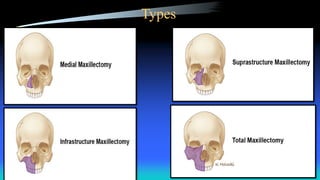
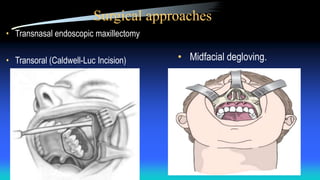


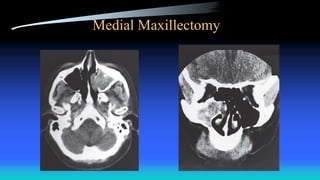



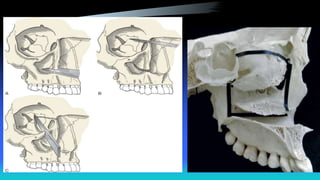







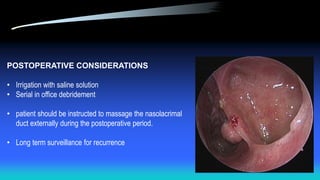
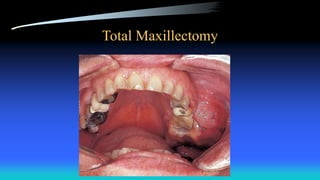




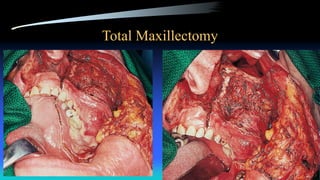





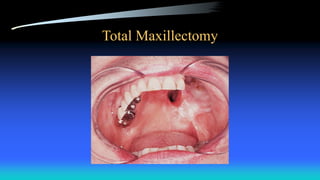
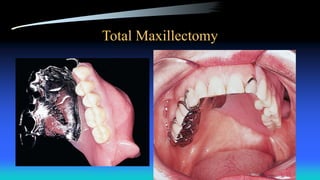
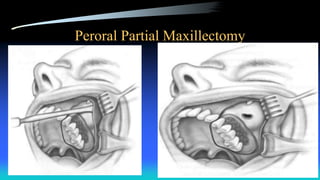
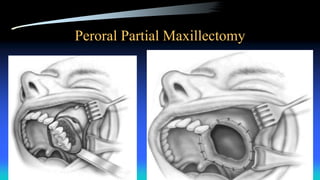

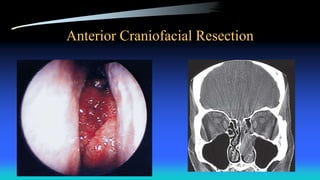
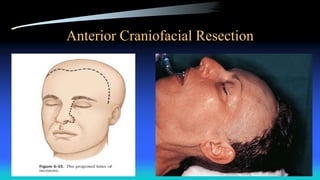

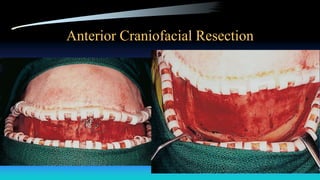
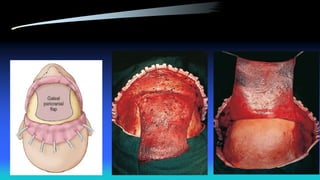
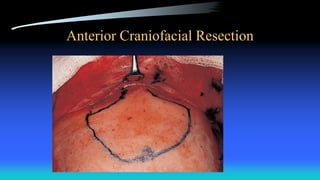
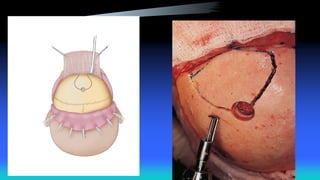
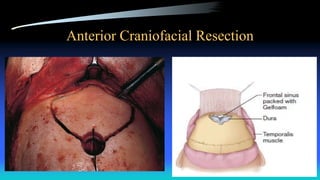
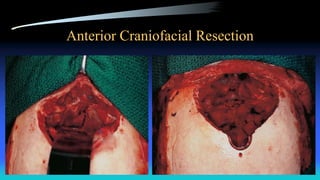
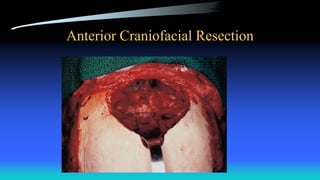
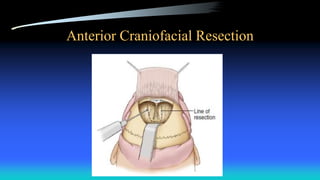
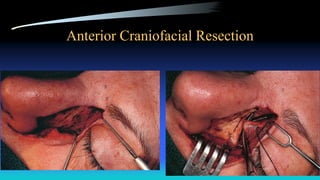
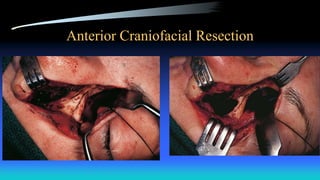
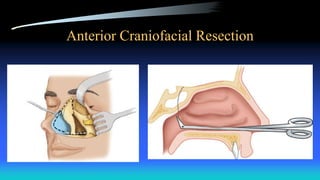
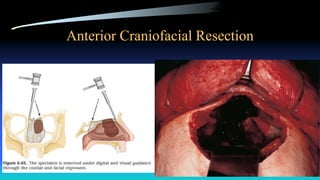
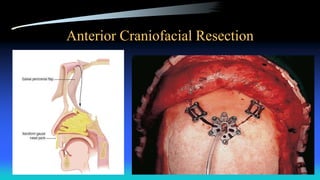

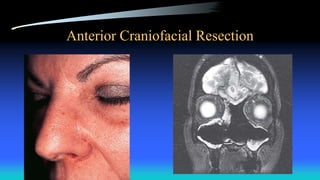




The document discusses maxillectomy and craniofacial resection, detailing surgical procedures for removing the maxilla bone due to tumors, infections, and other conditions. It outlines indications, contraindications, various surgical approaches, preoperative evaluations, and postoperative considerations, as well as reconstruction options and complications associated with these procedures. Key surgical techniques include medial maxillectomy, total maxillectomy with orbital exenteration, and anterior craniofacial resection, emphasizing the importance of proper tumor assessment and reconstruction goals.























































































