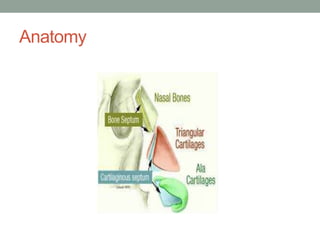
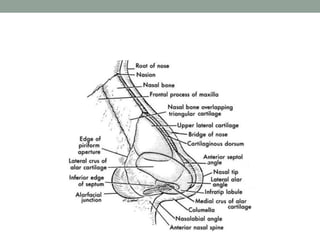
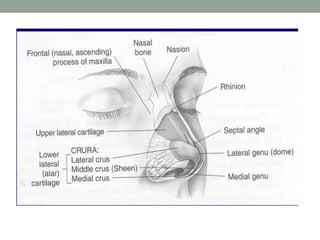
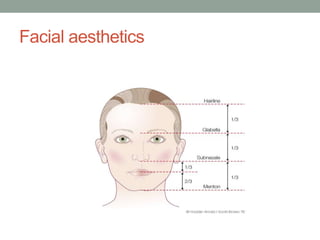
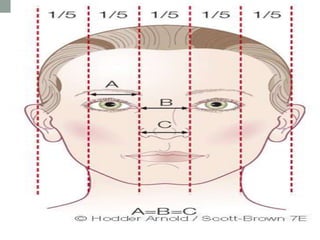
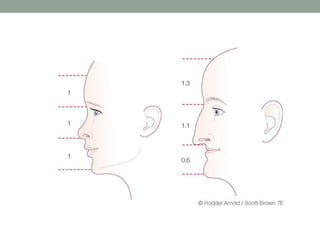
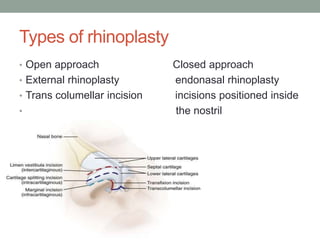
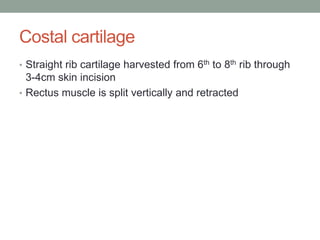
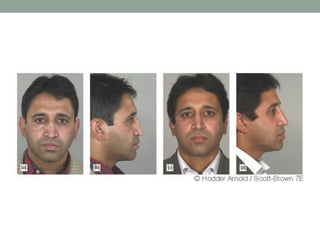
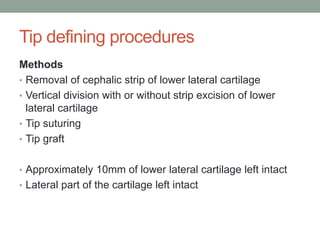
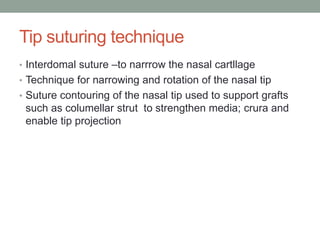
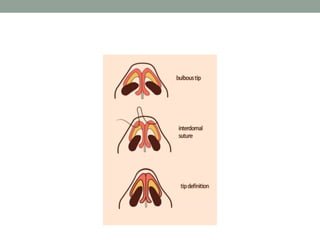
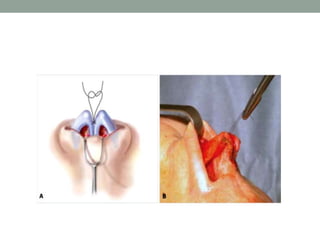
This document provides an overview of rhinoplasty procedures. It discusses the history and anatomy of rhinoplasty. It describes techniques for open and closed rhinoplasty approaches. It covers tip work including tip suturing and grafts. It also discusses nasal augmentation including graft materials and saddle nose repair. Deformities like deviated nose and underprojected tip are reviewed along with surgical correction methods. Key anatomical structures and surgical principles are emphasized.