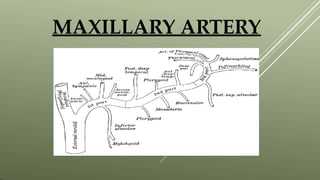
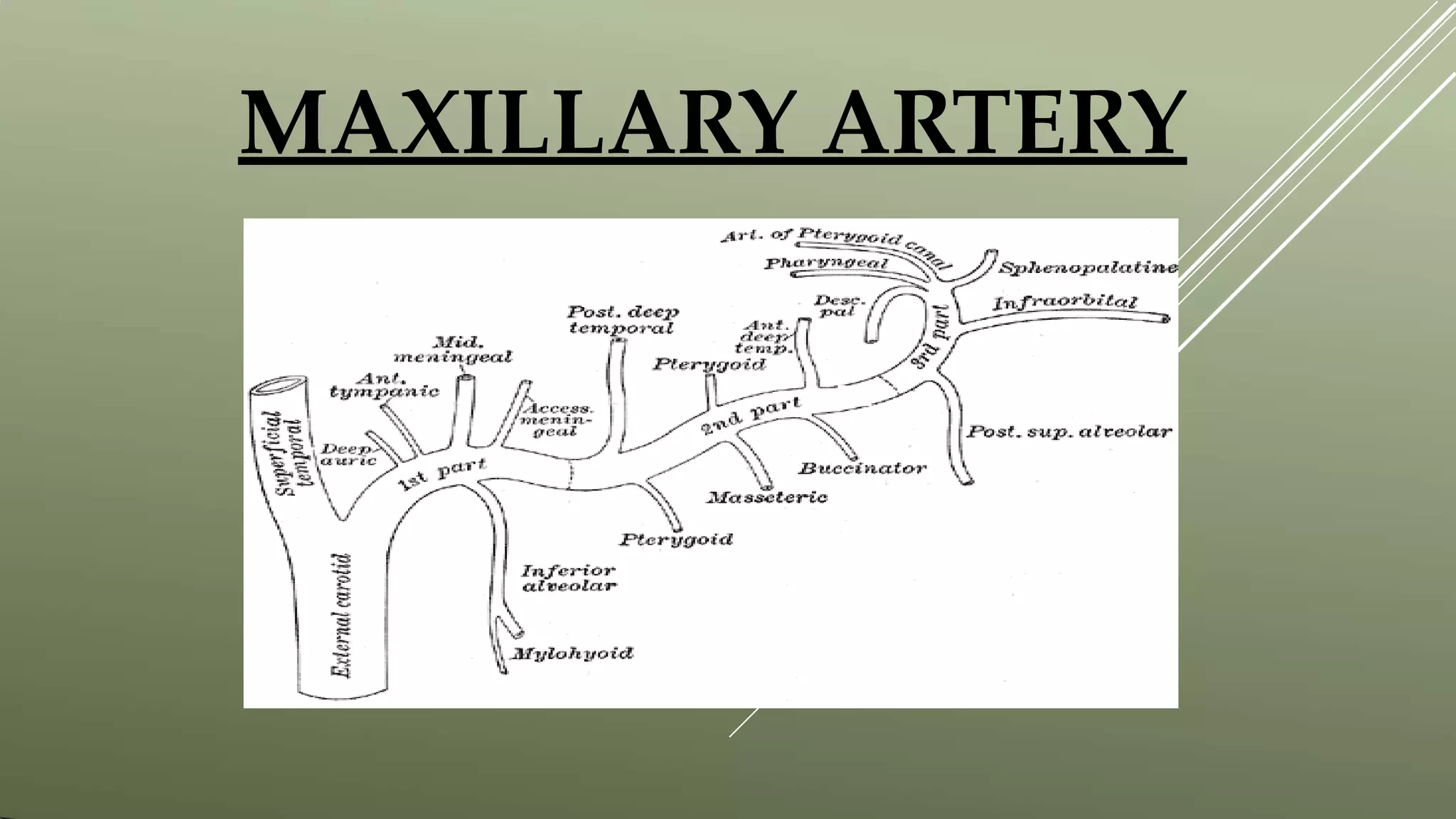
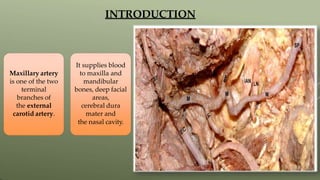
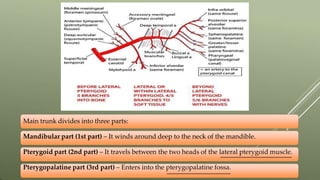
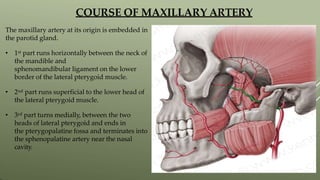
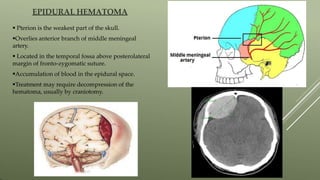
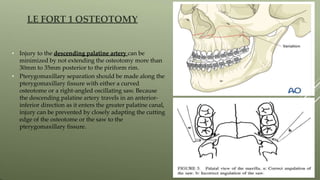
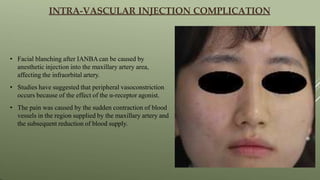
The maxillary artery arises from the external carotid artery and divides into three parts - the mandibular, pterygoid, and pterygopalatine parts. It supplies structures in the face and nasal cavity. The pterygoid plexus of vessels anastomoses with the facial vein and cavernous sinus, allowing for spread of infections. Injuries to branches of the maxillary artery can cause nosebleeds, epidural hematomas, or complications from surgery like Le Fort I osteotomies.

![REFERENCES
1. B.D Chaurasia’s Human Anatomy 6TH Edition.
2. Cunningham’s Manual of Practical Anatomy.
3. CHAPTER VI: Arteries, Gray’s Anatomy.
4. Images from KENHUB.COM.
5.Adriana L. Natali1; Vamsi Reddy2; Jonathan T. Leo3. Neuroanatomy, Middle
Meningeal Arteries [PUBMED].
6. Ekramul M. Gofur1; Yasir Al Khalili2. Anatomy, Head and Neck, Internal
Maxillary Arteries.
7.Sang-Hoon Kang and Yu-JinWon. Facial blanching after inferior alveolar nerve
block anesthesia: an unusual complication.
8. K K Li, J G Meara, A Alexander Jr. Location of the descending palatine artery in
relation to the Le Fort I osteotomy](https://image.slidesharecdn.com/maxillaryartery-210103043557-230614143711-fe4b1c75/85/maxillaryarter-pptx-29-320.jpg)
































![pterygopalatine_fossa_and_its_approachs[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pterygopalatinefossaanditsapproachs1-231217010847-cfbc0b0a-thumbnail.jpg?width=640&height=640&fit=bounds)















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






