Downloaded 84 times
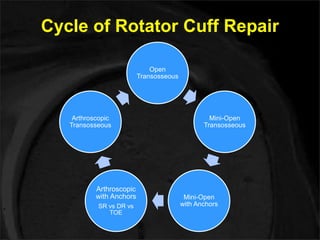
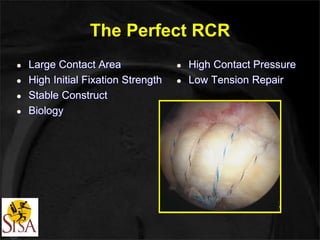

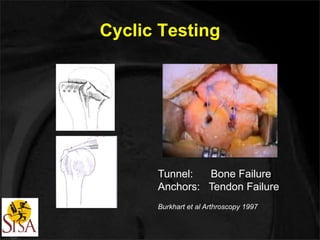
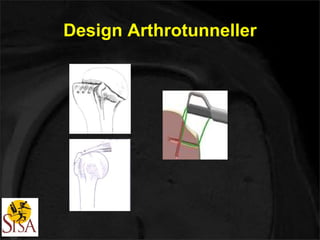




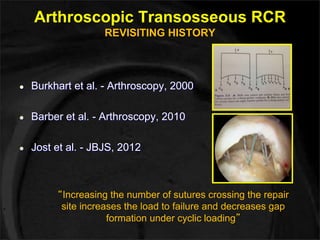
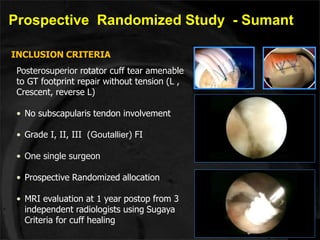
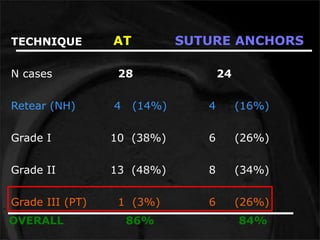
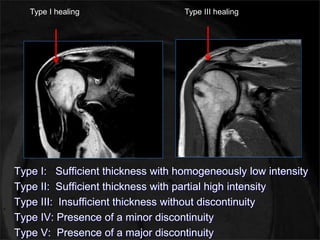
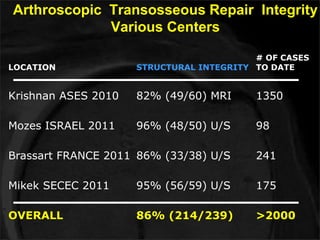
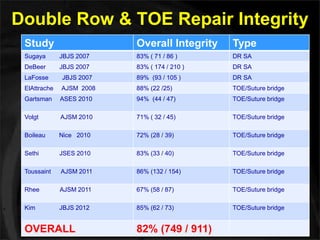
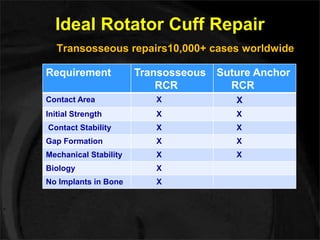
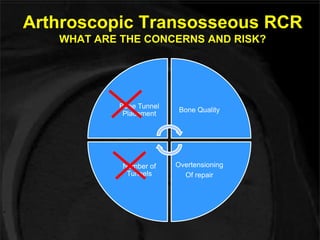
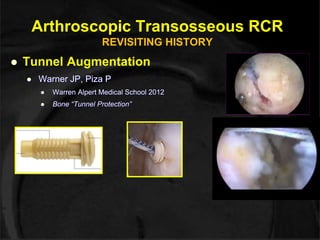
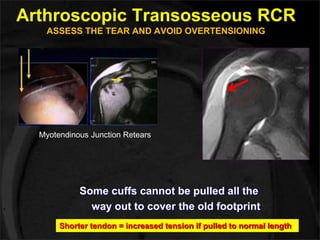
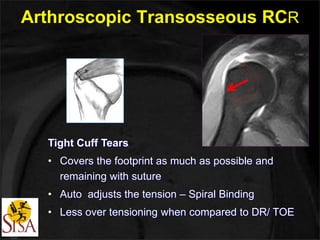
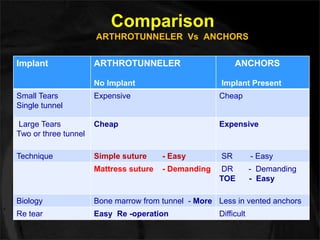
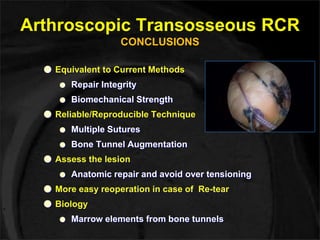



This document discusses arthroscopic transosseous rotator cuff repair. It begins with a brief history of rotator cuff repair techniques. It then describes the ideal properties of rotator cuff repair and how arthroscopic transosseous repair achieves high fixation strength, stability, and biology. The document outlines the surgical technique and presents clinical and biomechanical data supporting the procedure. It concludes that arthroscopic transosseous repair provides equivalent outcomes to current anchor-based techniques with benefits including no implants, multiple sutures, and potential for easier revision surgery.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)