

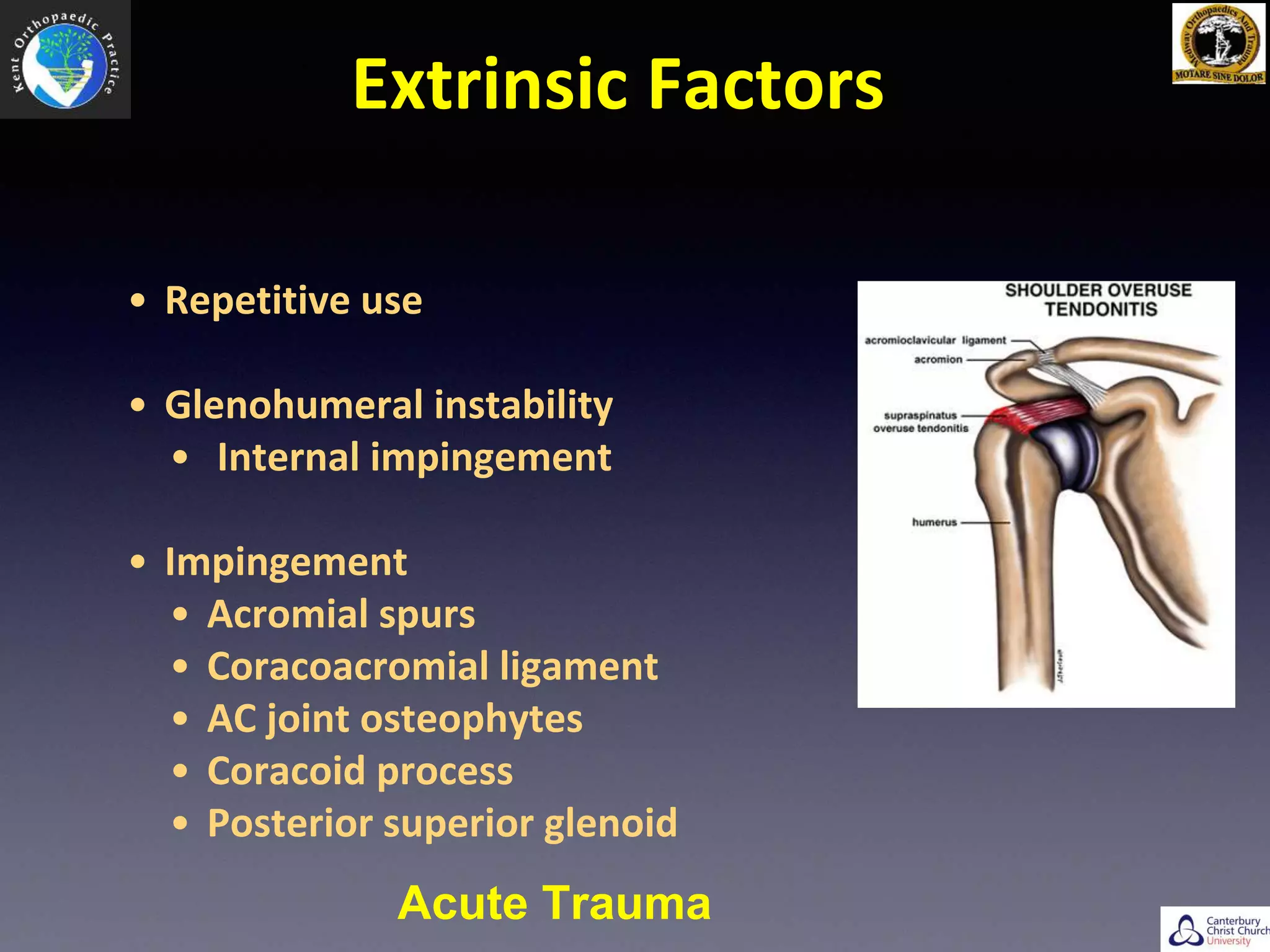





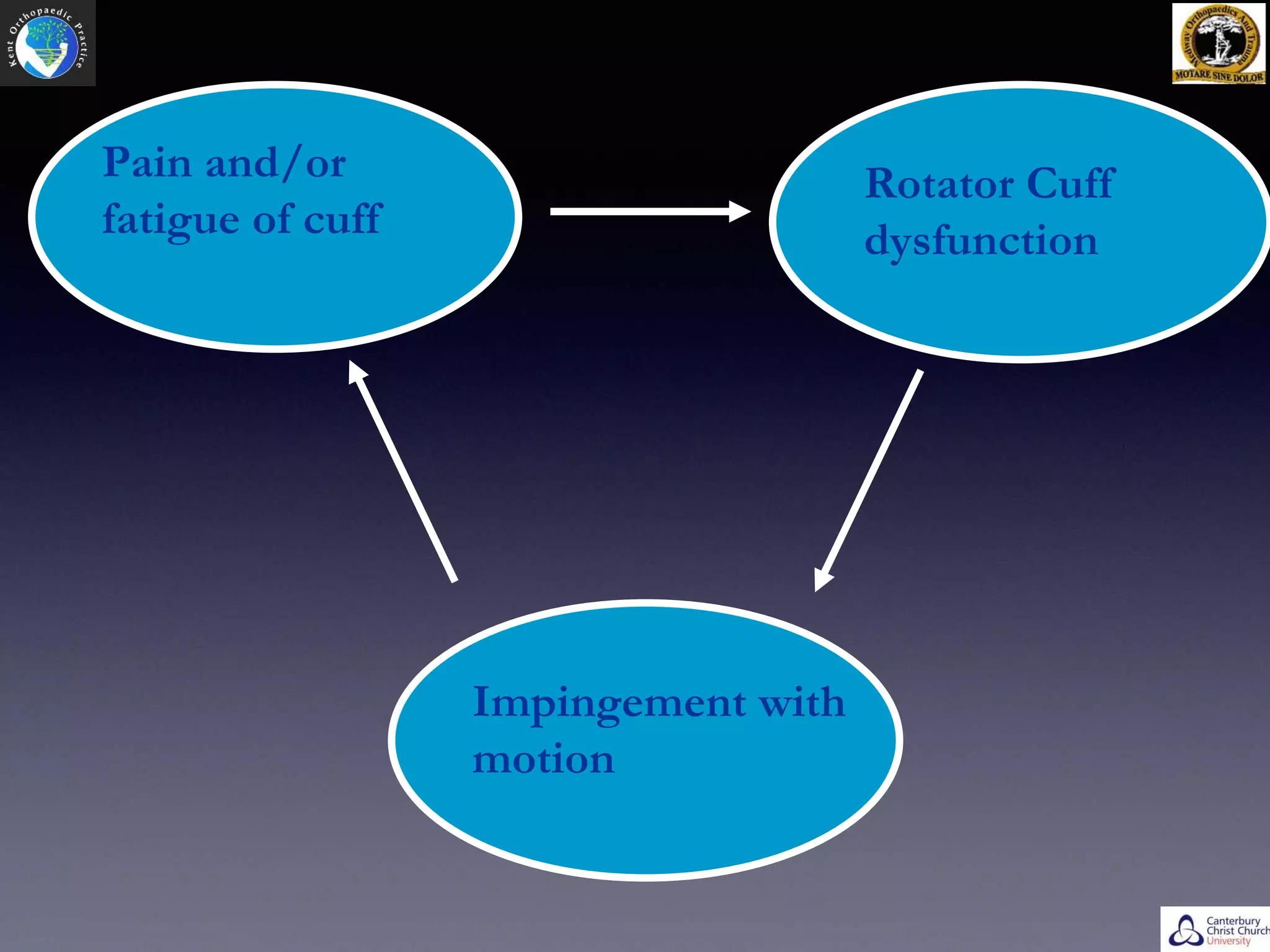

























- Rotator cuff tears can be caused by extrinsic factors like repetitive use or impingement, or intrinsic factors like changes in tendon vascularity or degenerative changes. - Physical examination involves inspection, palpation, range of motion testing and muscle strength testing. Investigations include ultrasound and MRI. - Symptomatic rotator cuff tears tend to increase in size over time if left untreated, especially in younger patients under 60 years old. - Surgery is indicated for failed conservative treatment, significant weakness, or acute tears in young active patients. - Arthroscopic repair has advantages over open repair like less pain and blood loss, but requires special instruments and equipment. -




![ROTATOR CUFF[4273].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rotatorcuff4273-221222051719-751991ae-thumbnail.jpg?width=640&height=640&fit=bounds)






































































