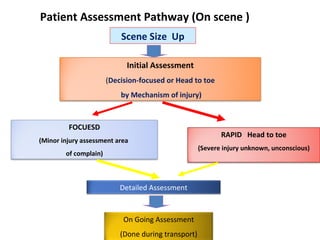
Patient Assessment Pathway(On scene )
Scene Size Up
Initial Assessment
(Decision-focused or Head to toe
by Mechanism of injury)
FOCUESD
(Minor injury assessment area
of complain)
RAPID Head to toe
(Severe injury unknown, unconscious)
Detailed Assessment
On Going Assessment
(Done during transport)
8.
Information : EMSReport
•Mechanism of injury
•Energy force involved
•Associated fracture
•Time of injury/ NPO
•Location of injury
Signs and symptomsof PBI
• skull or facial fractures,
• burns to more than 10% of total body surface area
(TBSA)
• penetrating head or chest wounds.
• Rapid shallow respirations are characteristic of lung
PBI, with shortness of breath (SOB)
• Dry or moist cough,
• Chest pain (often retrosternal)
• Diminished breath sounds.
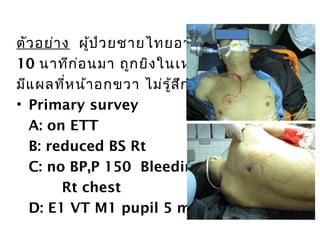
ตัวอย่ำง ผู้ป่วยชำยไทยอำยุ 40ปี
10 นำทีก่อนมำ ถูกยิงในเหตุกำรณ์ชุมนุม
มีแผลที่หน้ำอกขวำ ไม่รู้สึกตัว มูลนิธินำำส่ง
• Primary survey
A: on ETT
B: reduced BS Rt
C: no BP,P 150 Bleeding from GSW
Rt chest
D: E1 VT M1 pupil 5 mm fixed BE
20.
Triage
Multiple casualties
= thenumber and severity of the injuries
Do not exceed the ability of the facility to render
care.
Treat life-threatening injuries first.
21.
Triage
Mass casualties
= thenumber and severity of the injuries exceed
the capability of the facility and staff.
The greatest chance of survival, with the least
expenditure of time, equipment, supplies, and
personnel are managed first.
Clinical Management Keys
Organizedteam approach with doing initial
assessment, coordinating procedures and
investigations
High priority multiple injury : ABC and impending
herniation
Low priority multiple injury : neuro, cardiac,
abdominal, severe chest injury, msk, burns
ED phase
24.
Clinical Management Keys
Treatbefore diagnosis in critically ill
Through physical examination for injuries
Frequent re-assessment
Monitoring vitals, intake/output, serial
Hb/Lactate, CVP and Swan Ganz, art line
ED phase
Resuscitation
•Protect and secureairway
•Oxygenation and ventilation
•Stop bleeding
•Vigorous shock therapy
•Protect from hypothermia
28.
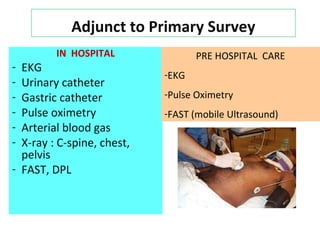
Adjunct to PrimarySurvey
IN HOSPITAL
- EKG
- Urinary catheter
- Gastric catheter
- Pulse oximetry
- Arterial blood gas
- X-ray : C-spine, chest,
pelvis
- FAST, DPL
PRE HOSPITAL CARE
-EKG
-Pulse Oximetry
-FAST (mobile Ultrasound)
29.
Trauma Life Support/ Advance Trauma care
Secondary survey
Mechanism of injury
Ample history
Physical examination : Head to toes
Complete neurologic examination
Adjuncts to secondary survey : Image
examination
Reevaluation
Clinical Management OfBlast Injury
• Management of pulmonary PBI is the same as
for pulmonary contusions
• Assume wheezing is due to pulmonary
contusion ; despite a history of asthma.
• Patients with penetrating trauma between the
nipples and scapulae there is a higher
probability for injury to great vessels and
mediastinal structures.1
• ECG should be performed for all chest pain
Key points
• Airemboloism
• Compartment Syndrome
• Early and subsequent chest X-ray (CXR)
• The combination of pulmonary infiltrates and
hypoxaemia defines pulmonary PBI. (gas exch
ange, using fewer tidal volume (TV) and press
ure changes )
44.
Key points
• Fowleror Trendelenburg positioning may
increase the risk of cerebral or coronary AAE.
• Massive haemoptysis may occur with
significant contusion