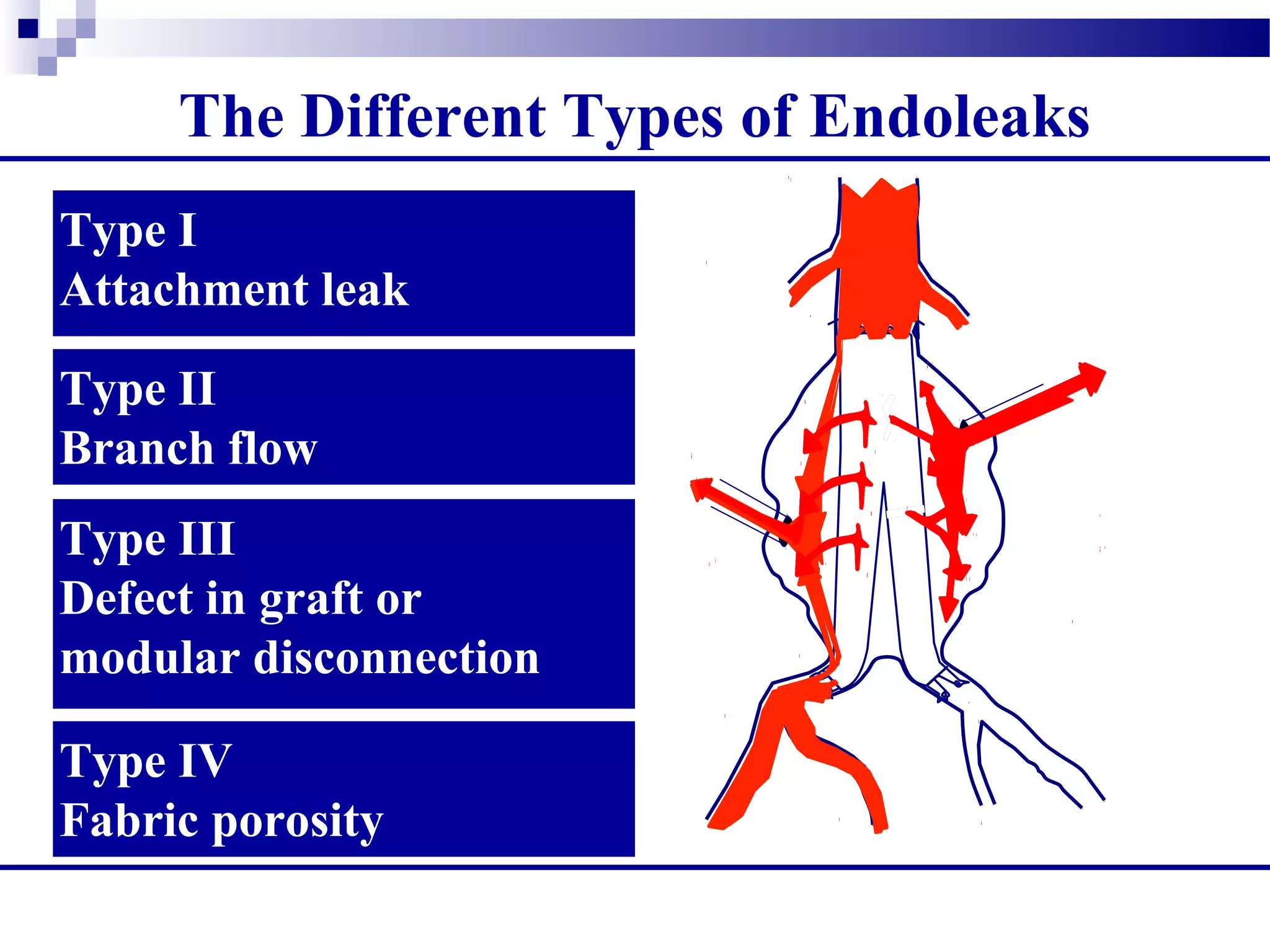
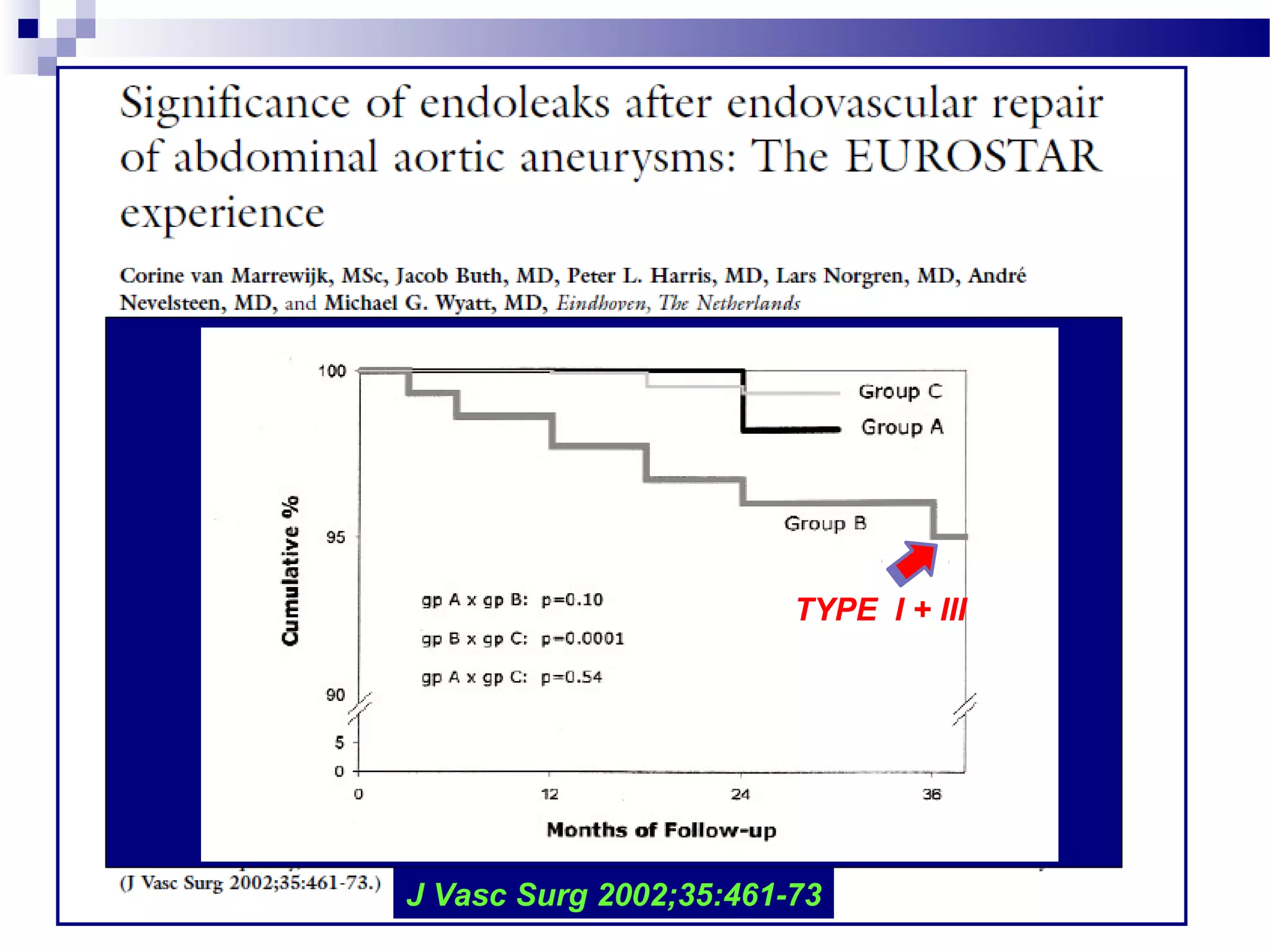
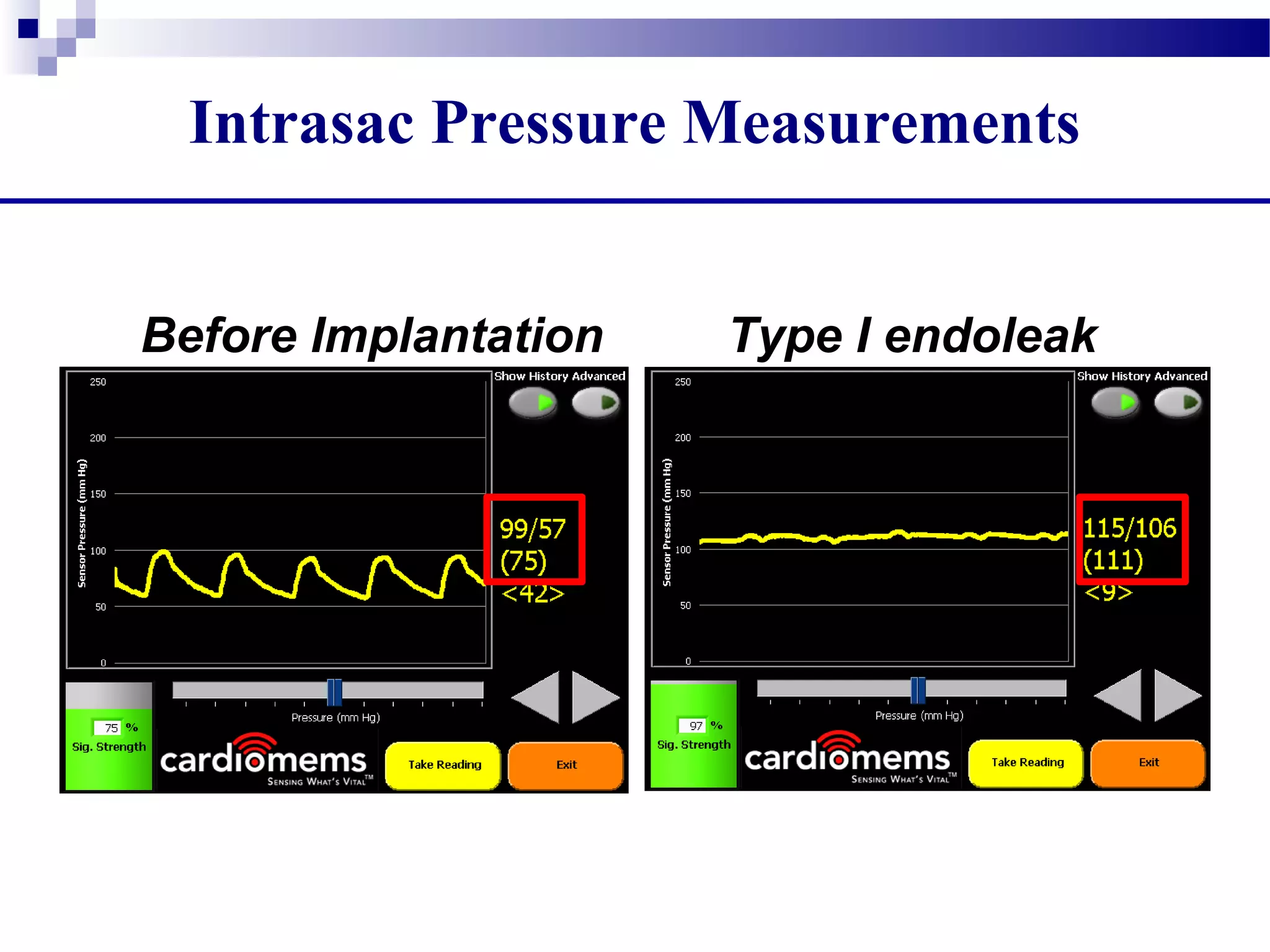
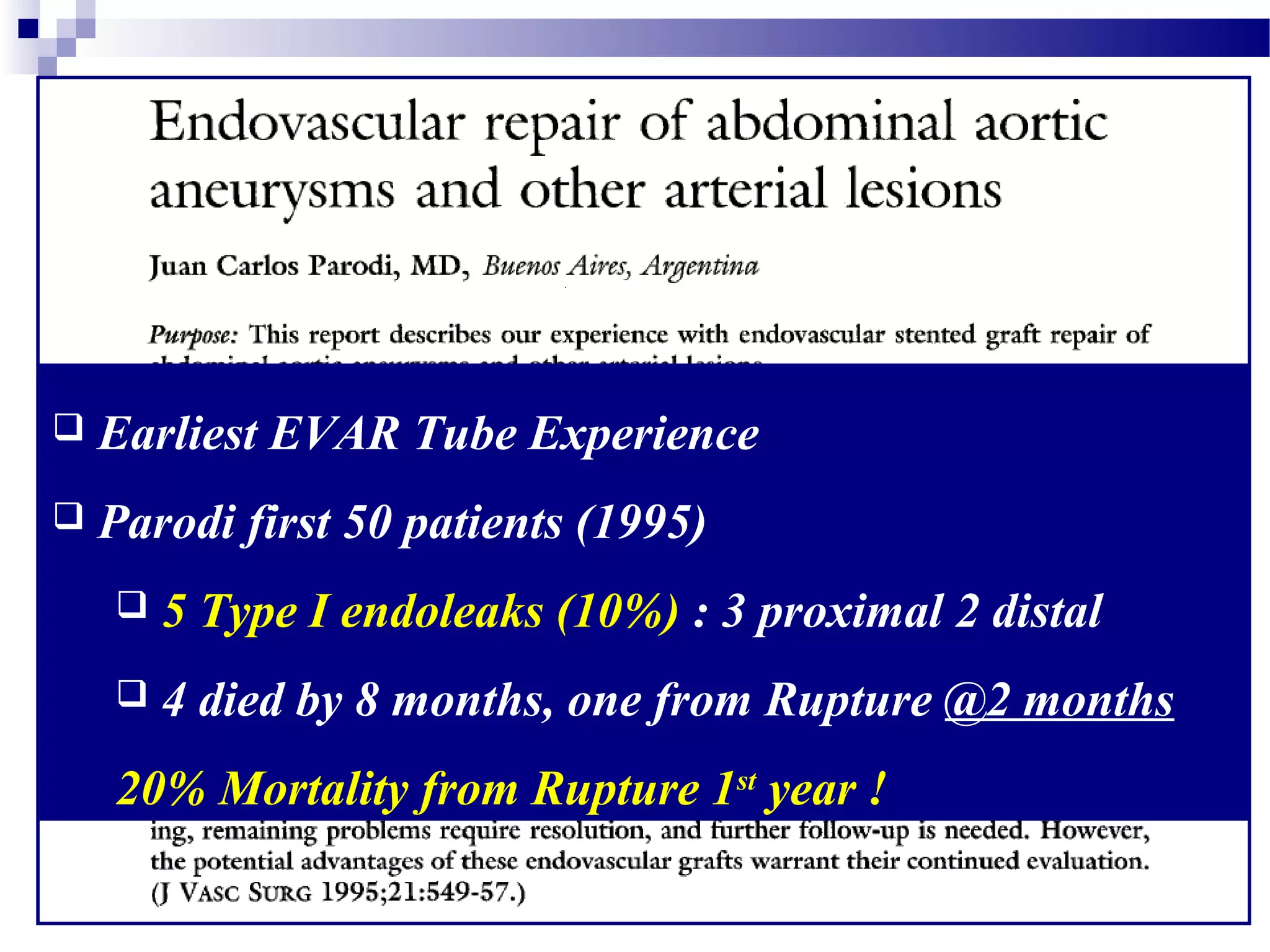
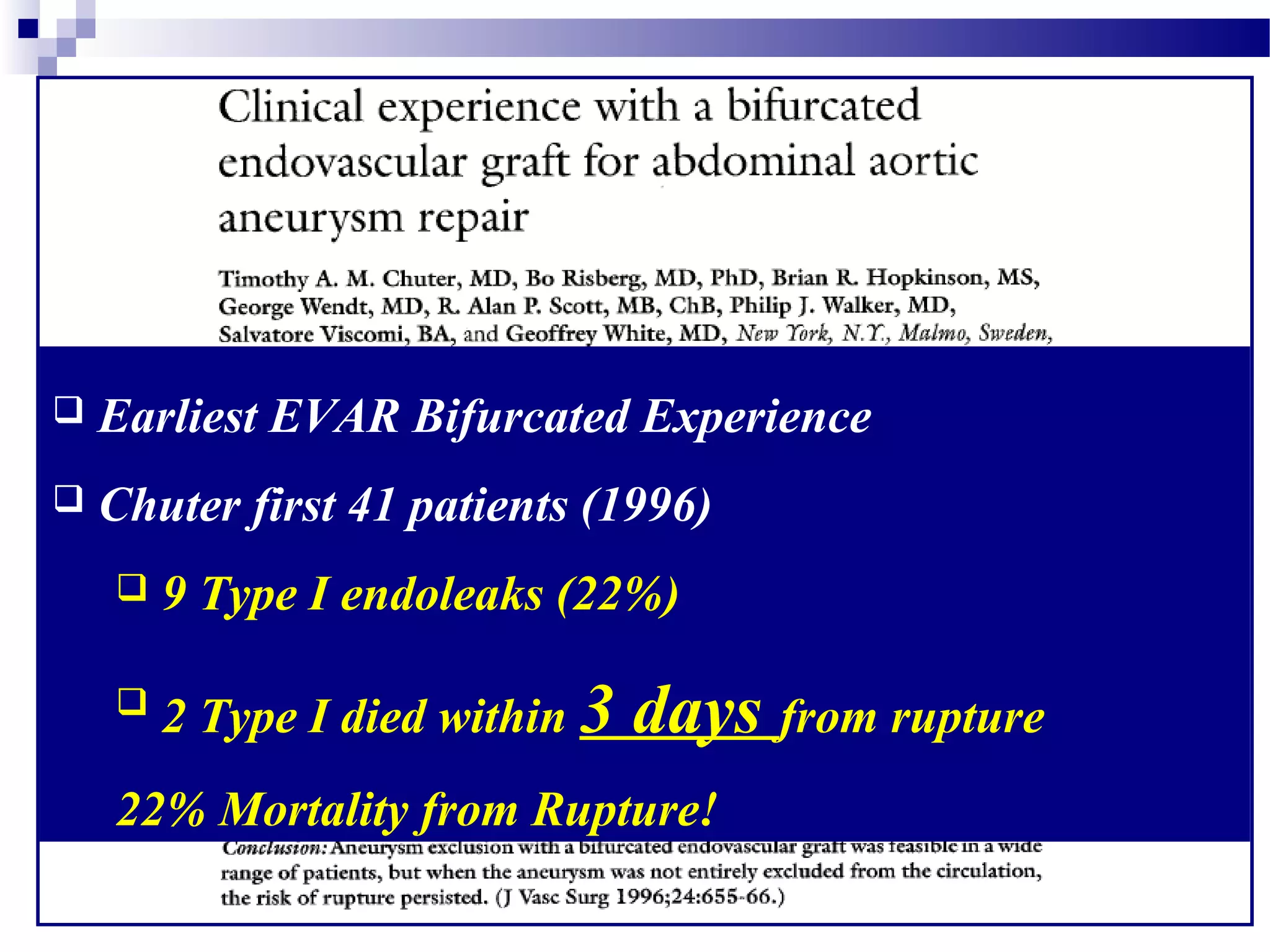
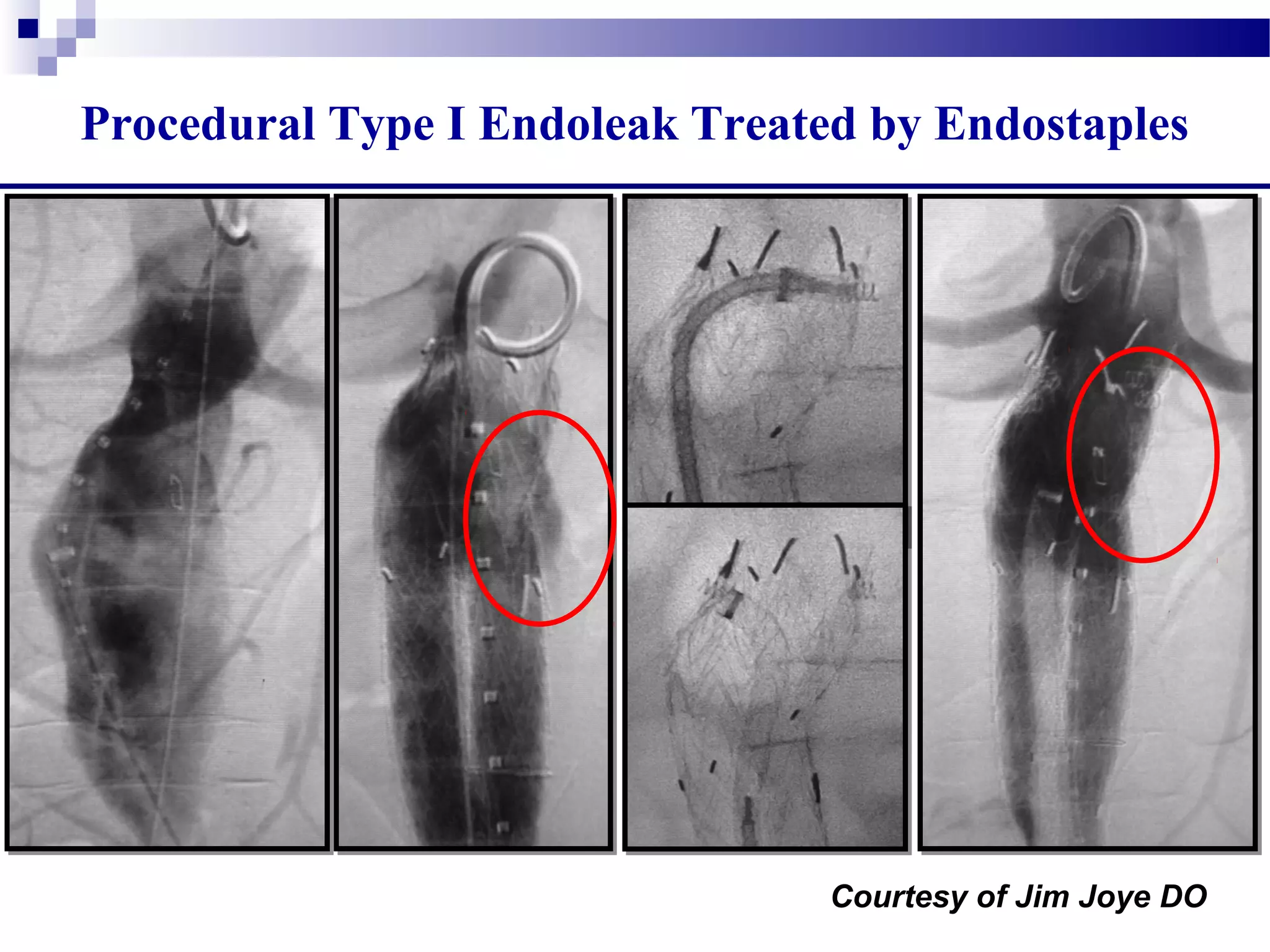
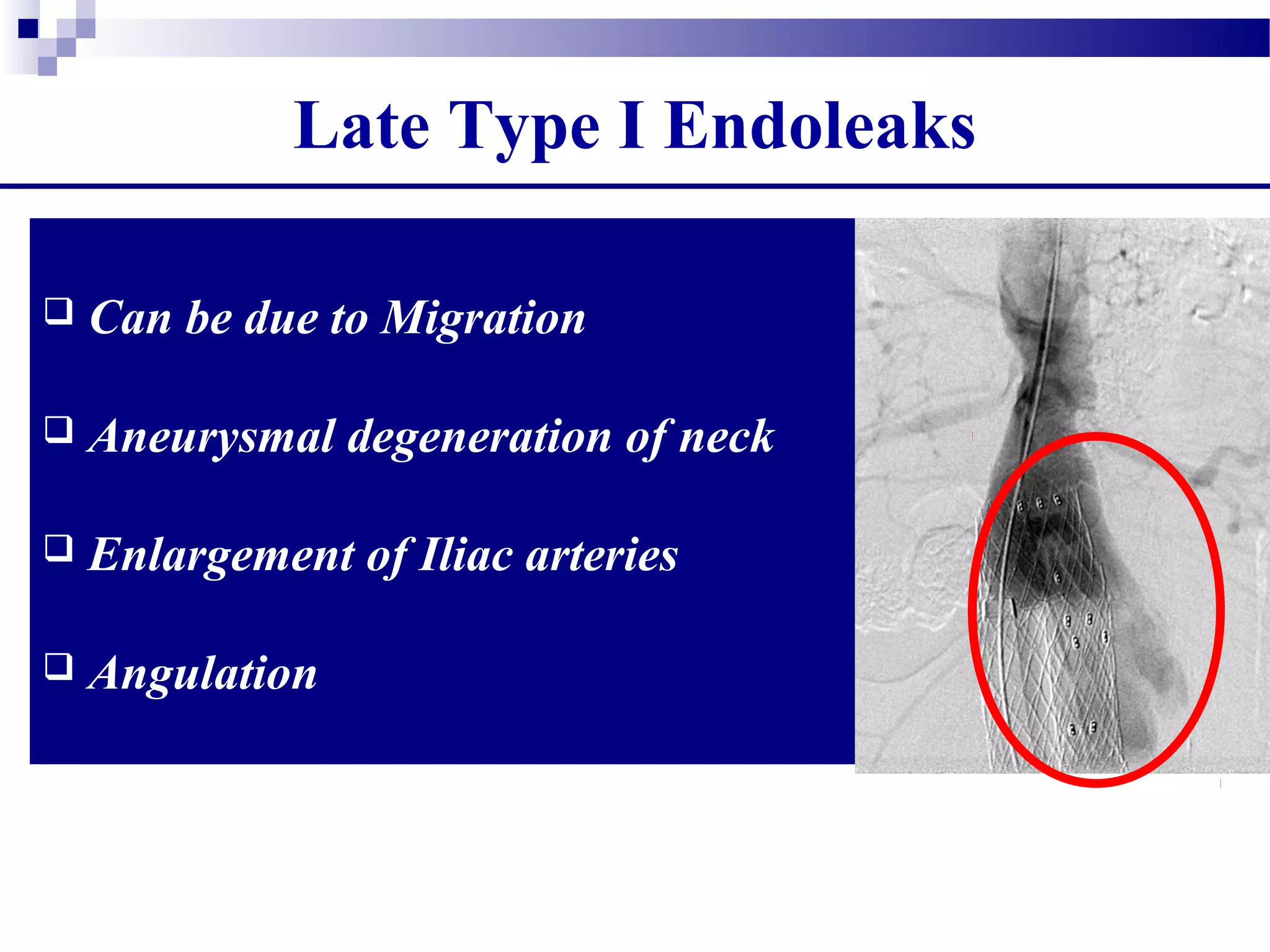
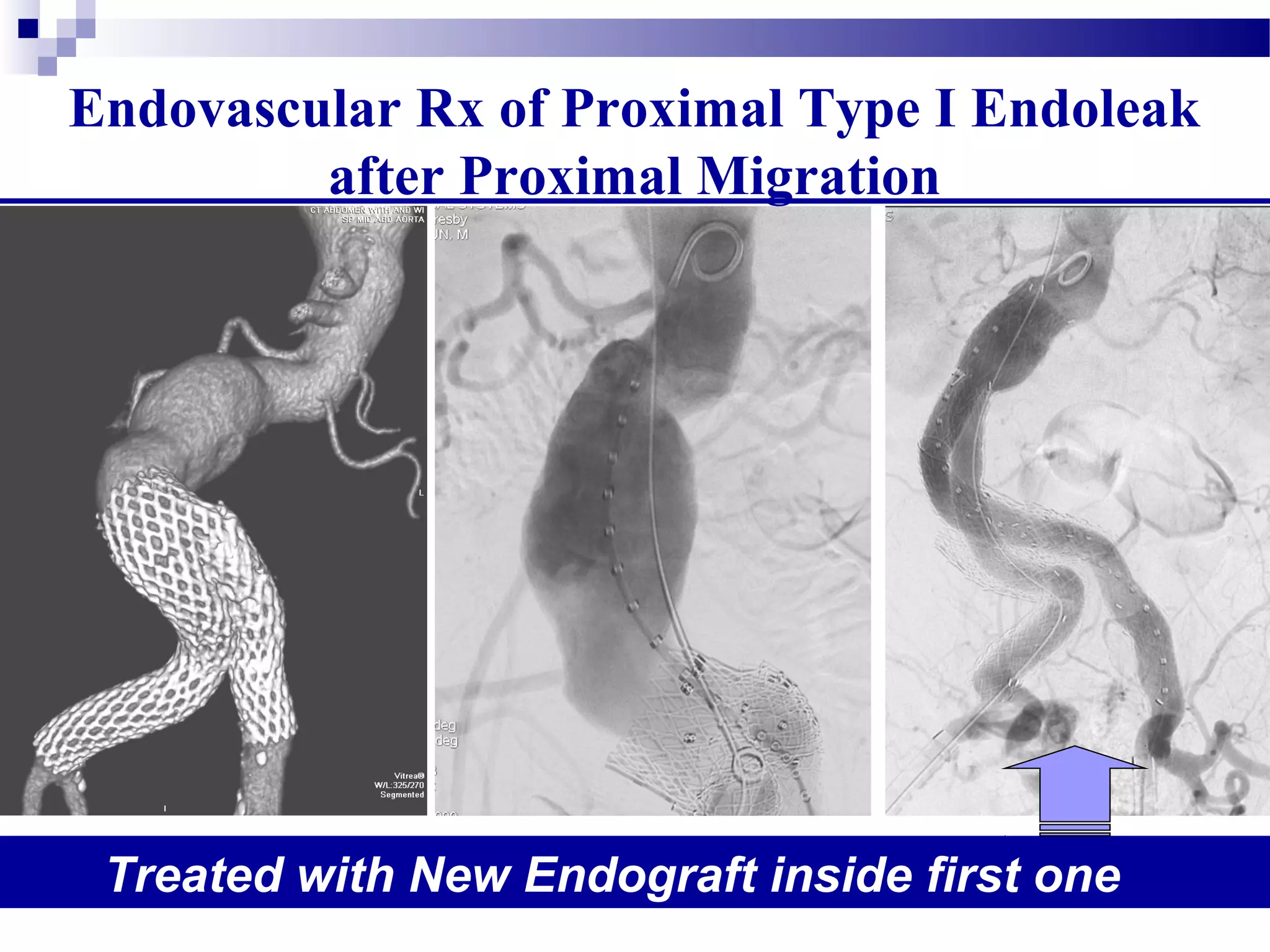
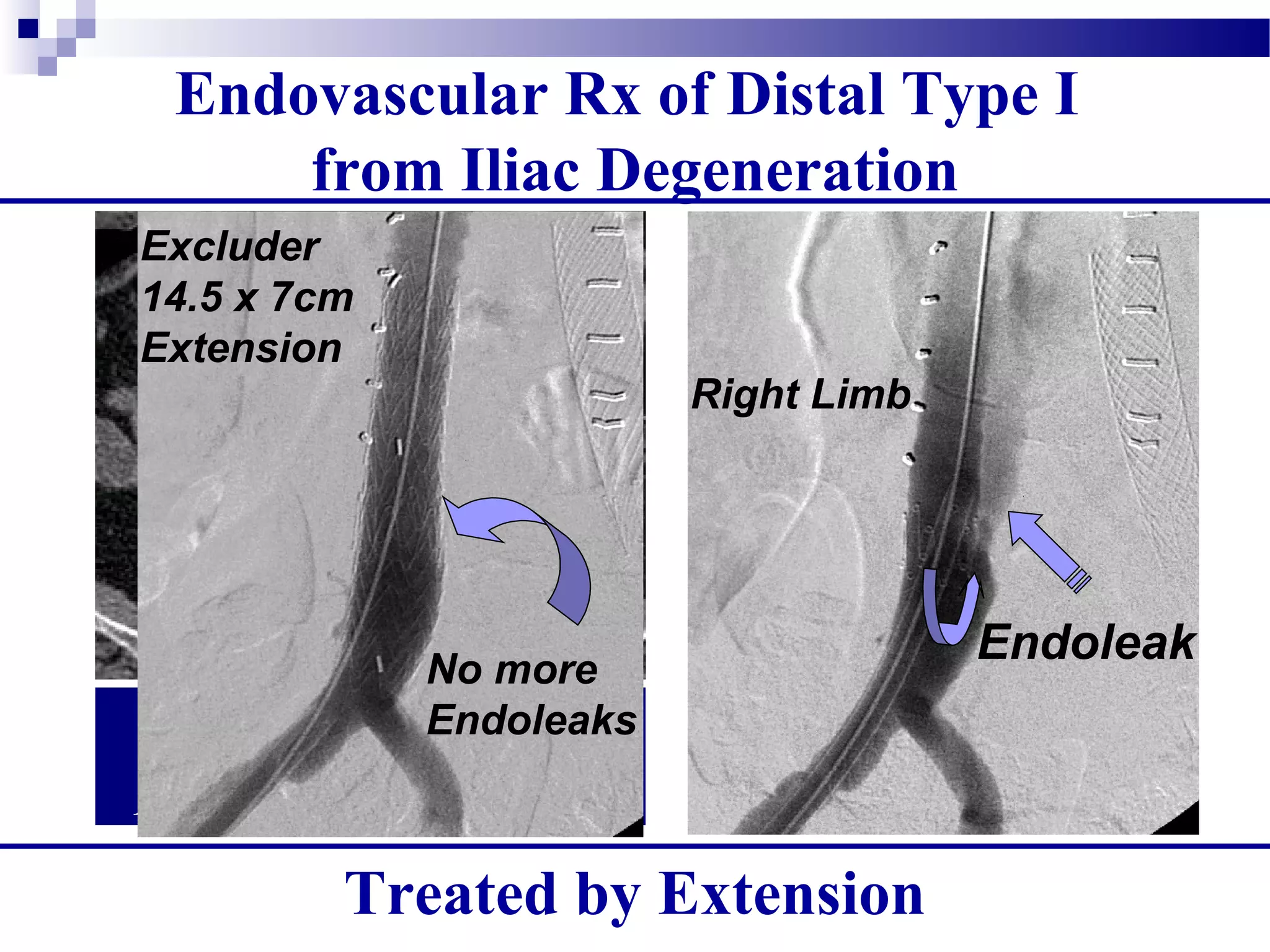
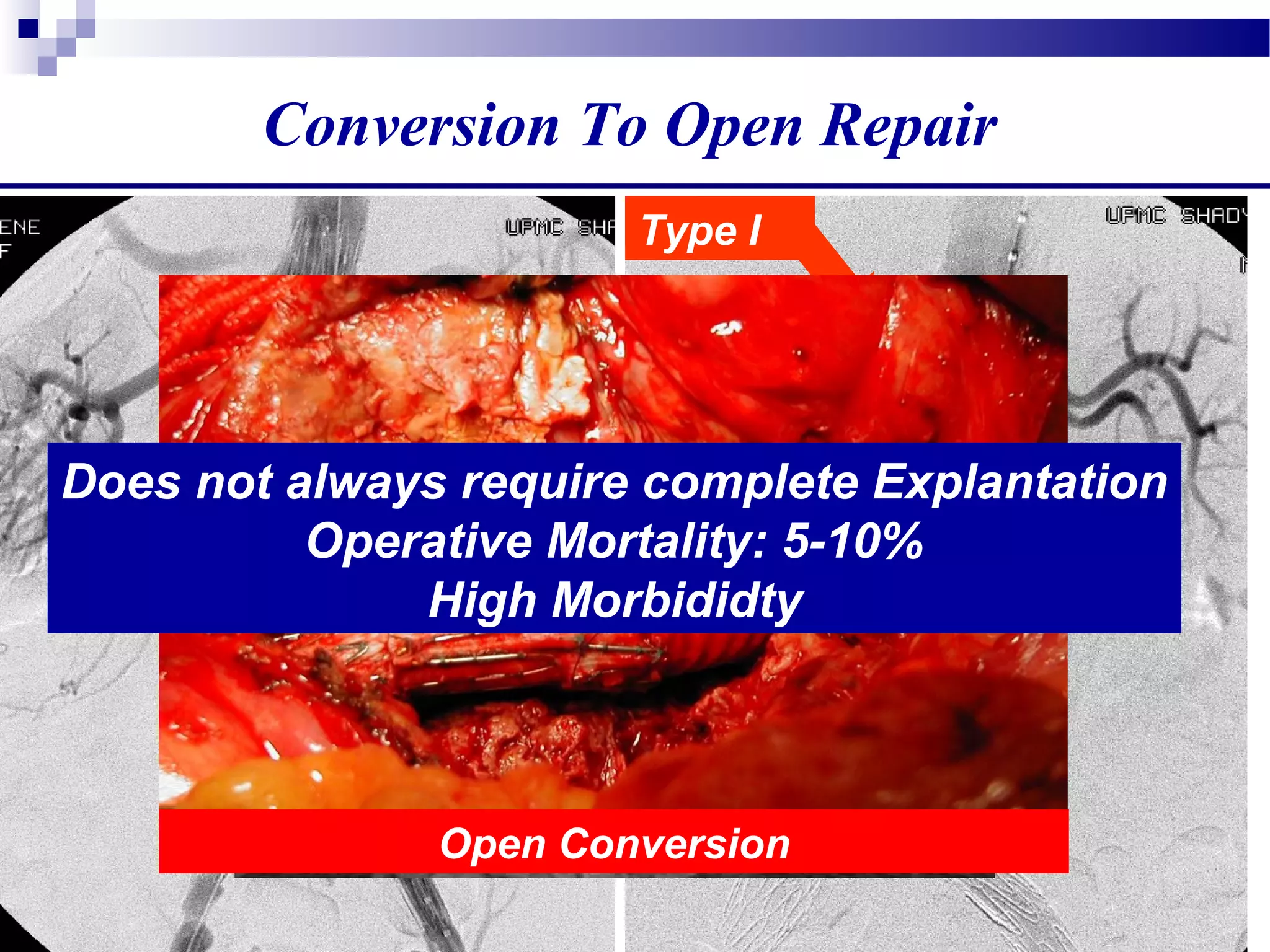
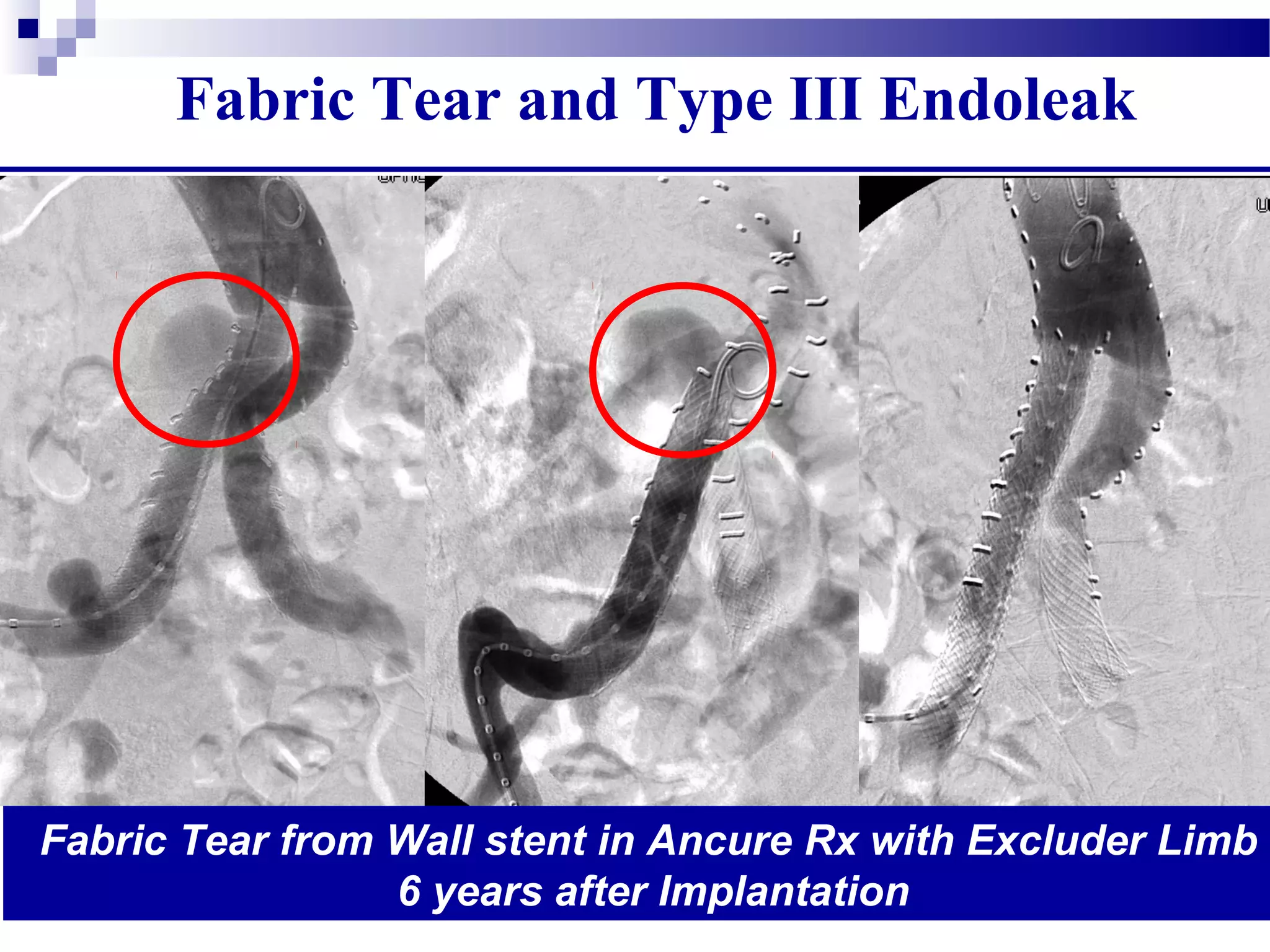
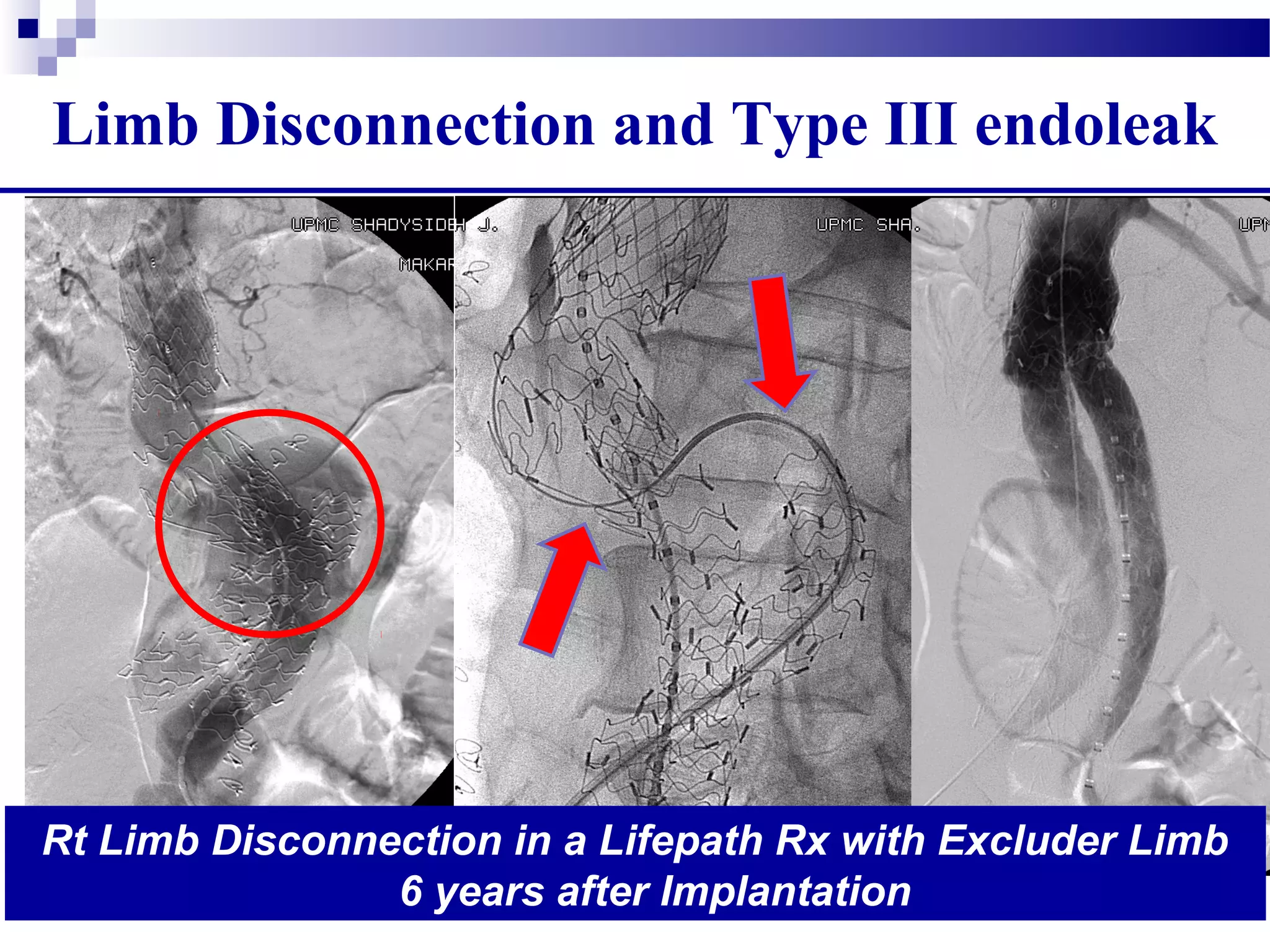
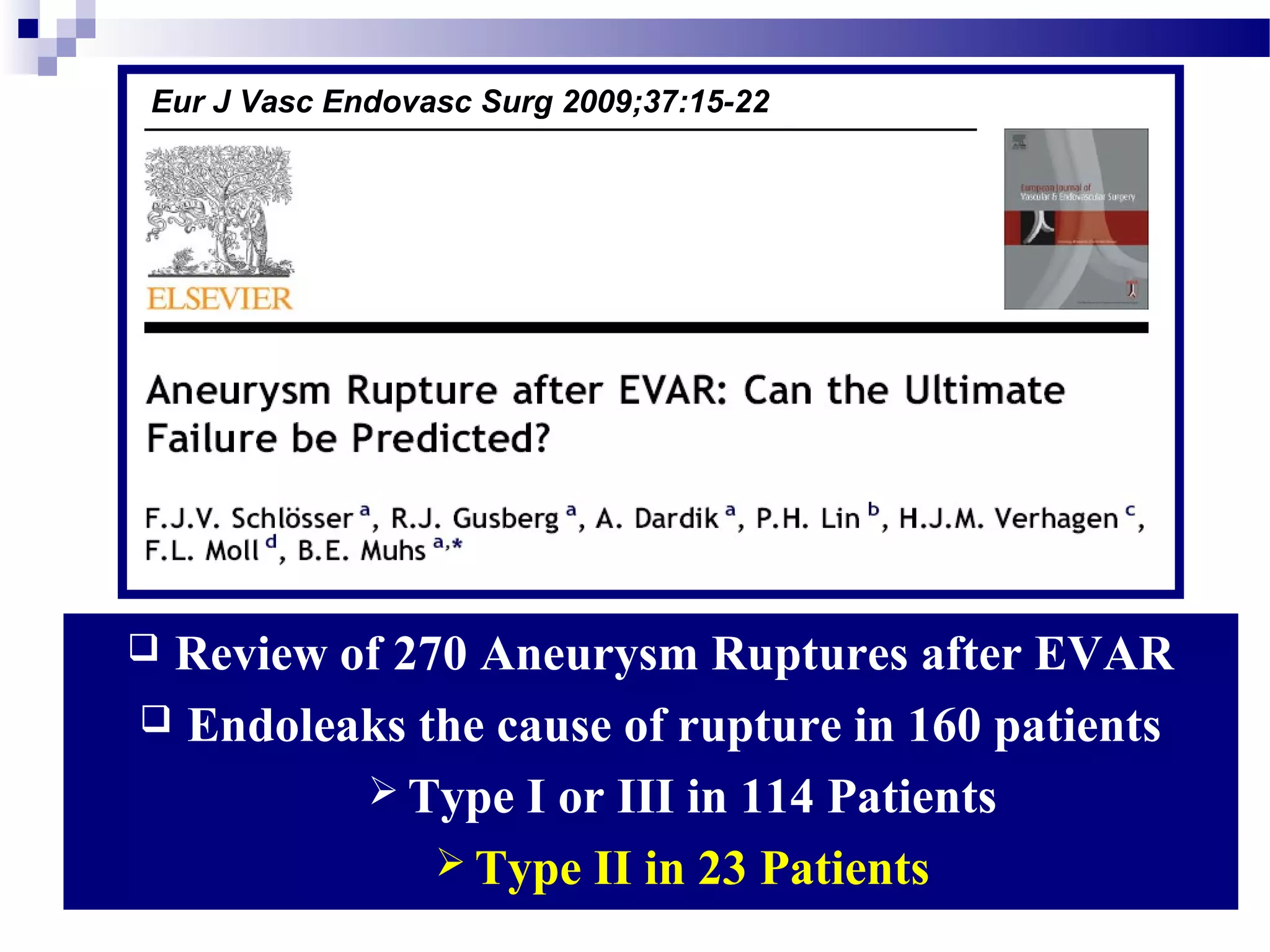
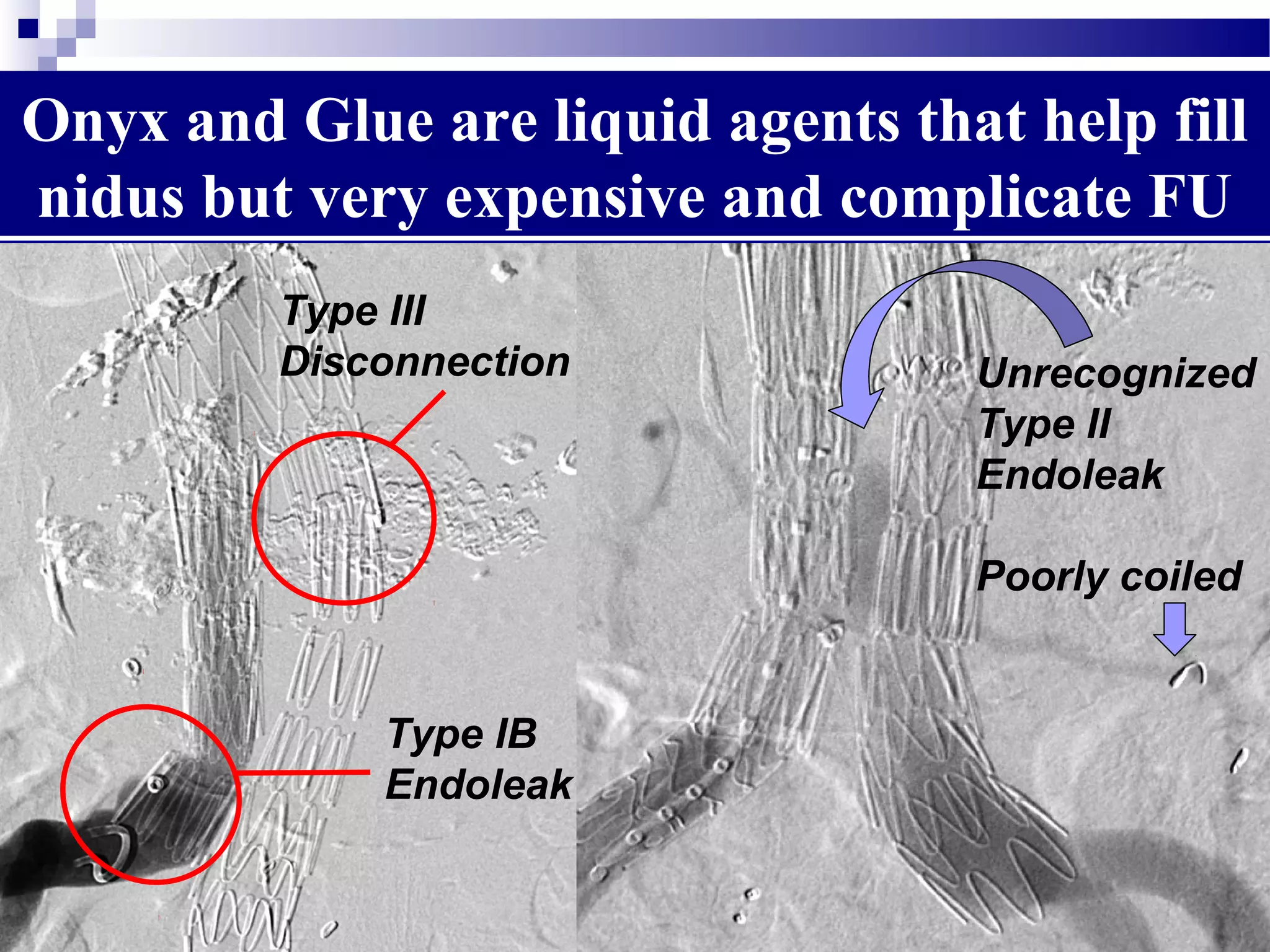
1. There are different types of endoleaks that can occur after EVAR, with Types I and III considered the most serious due to their risk of rupture if not treated.
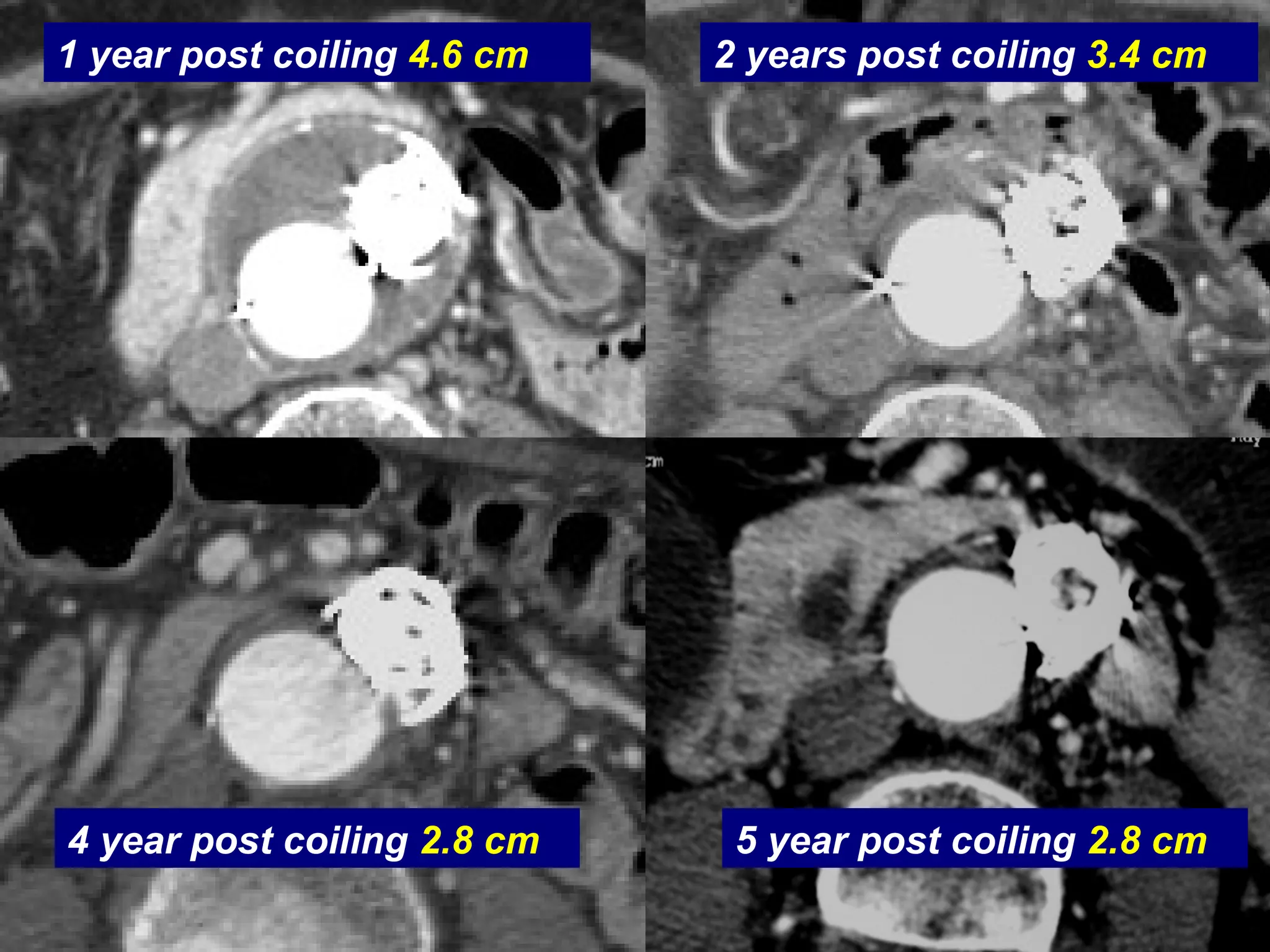
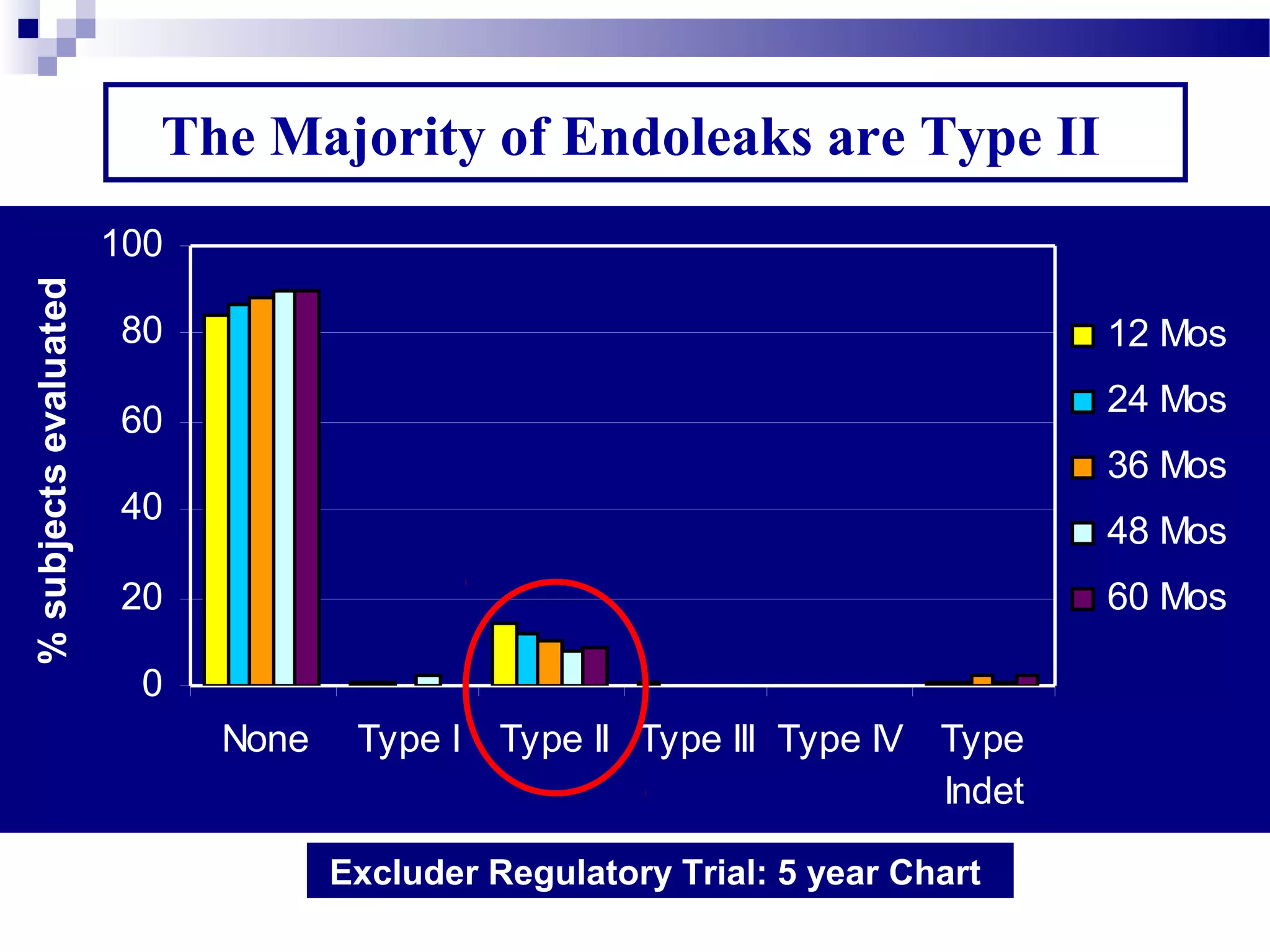
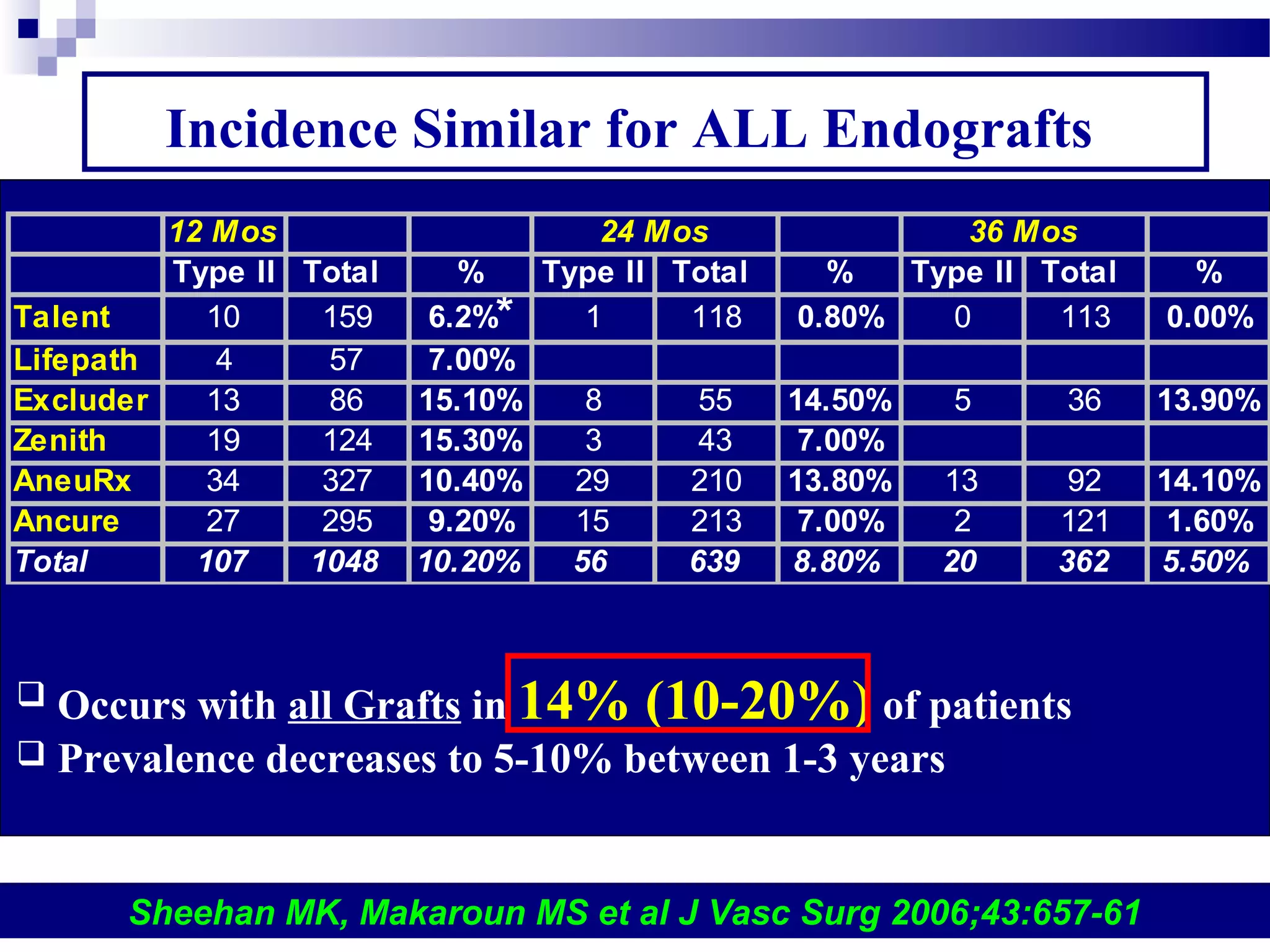
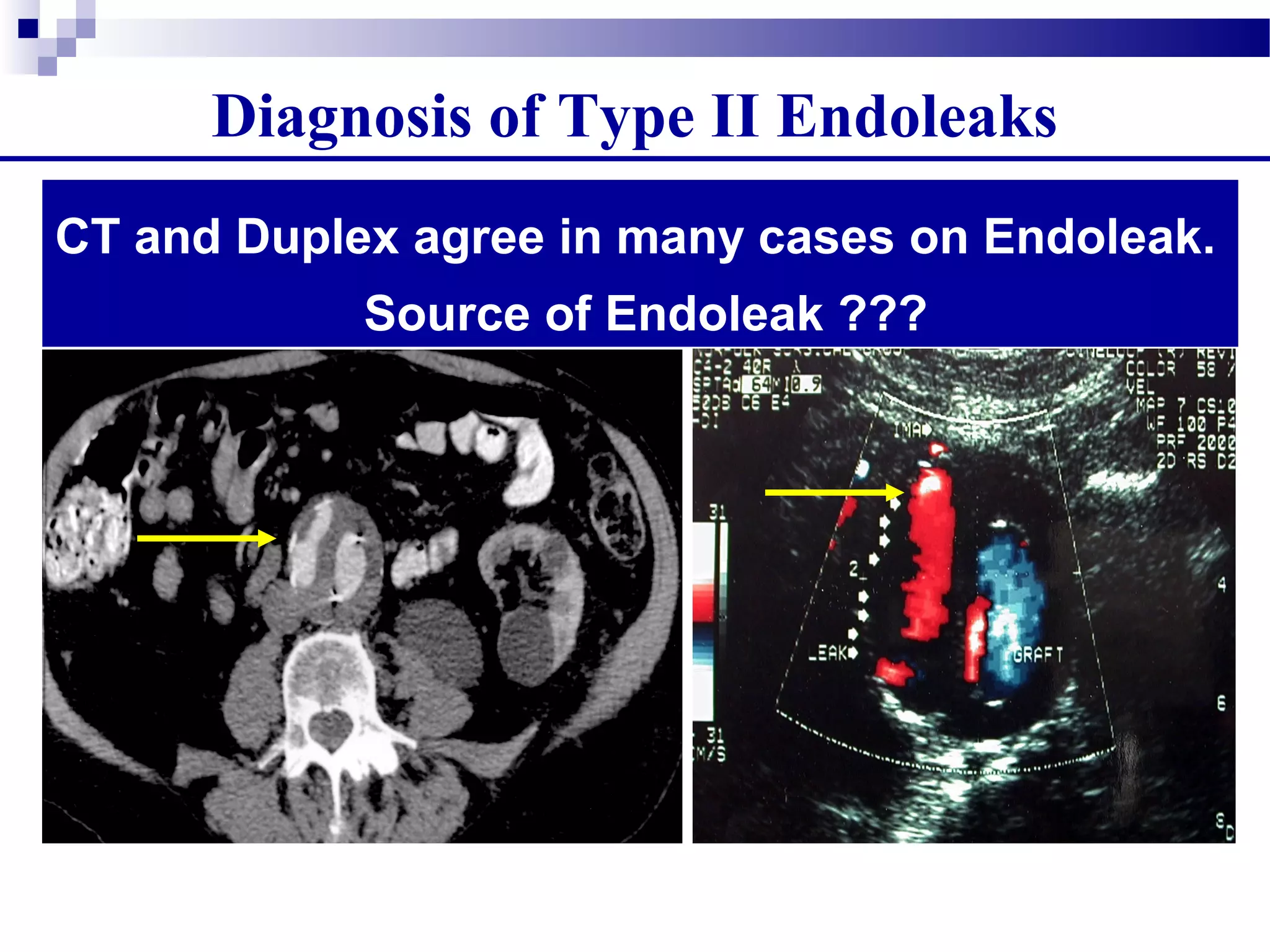
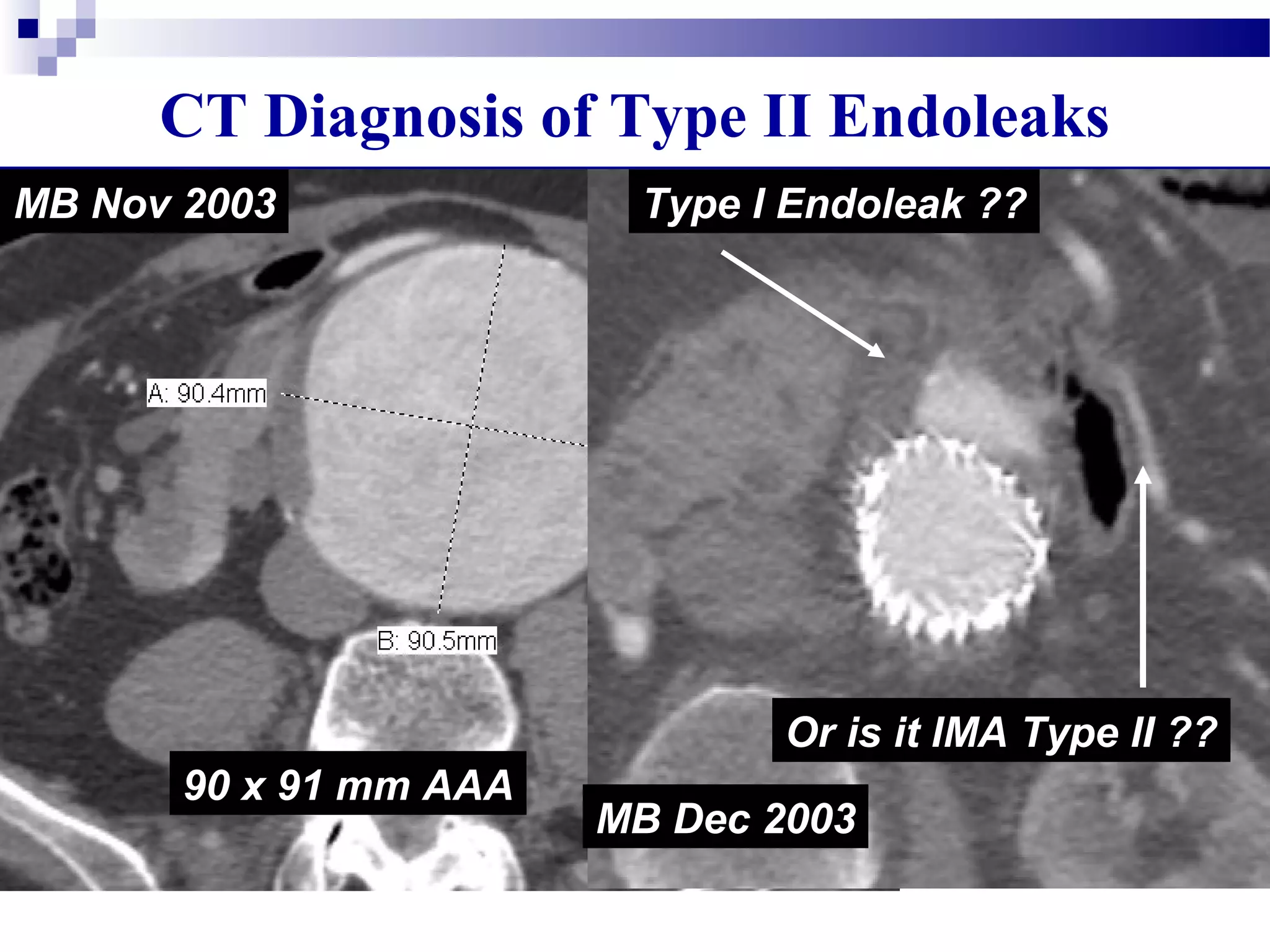
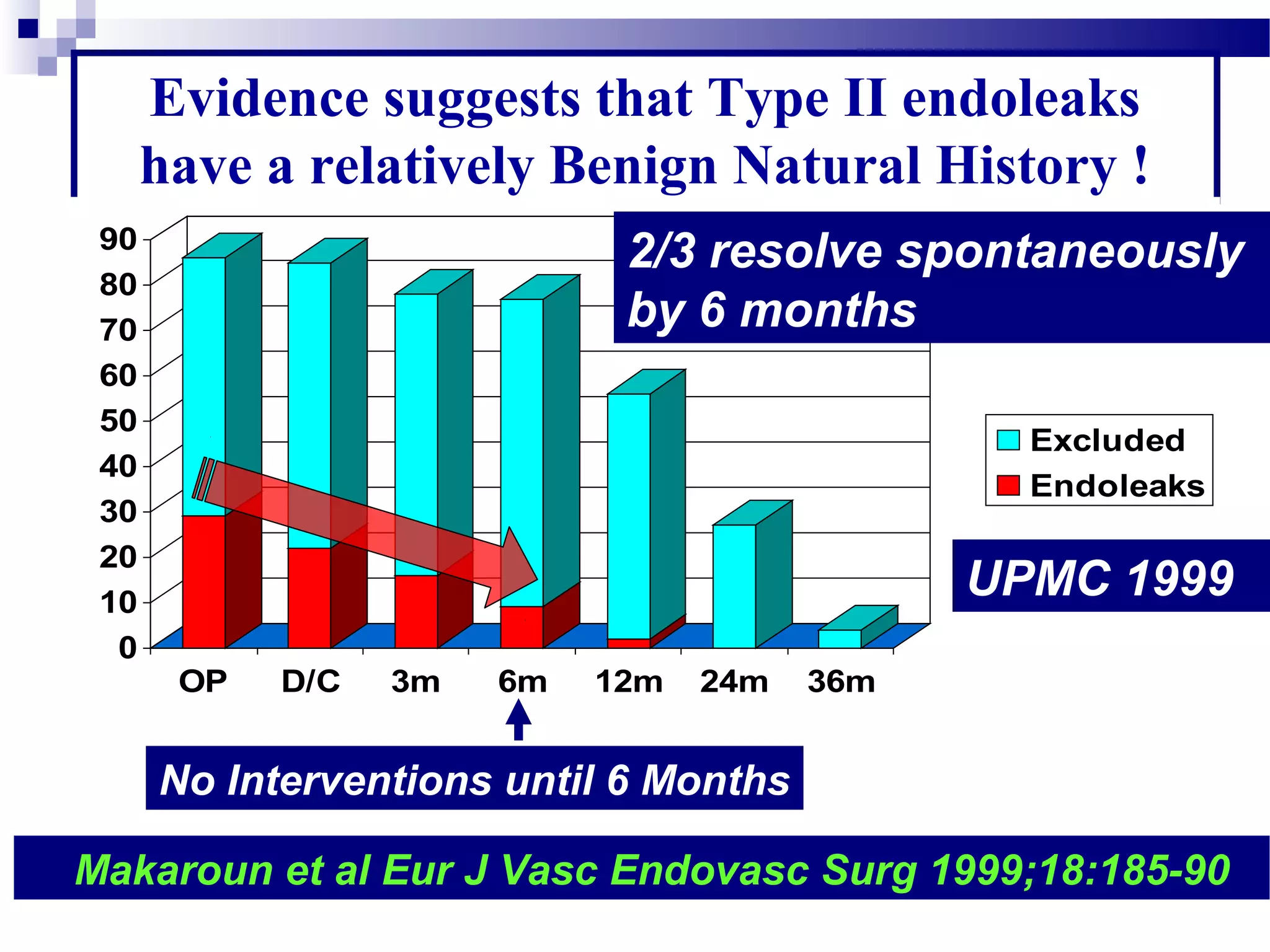
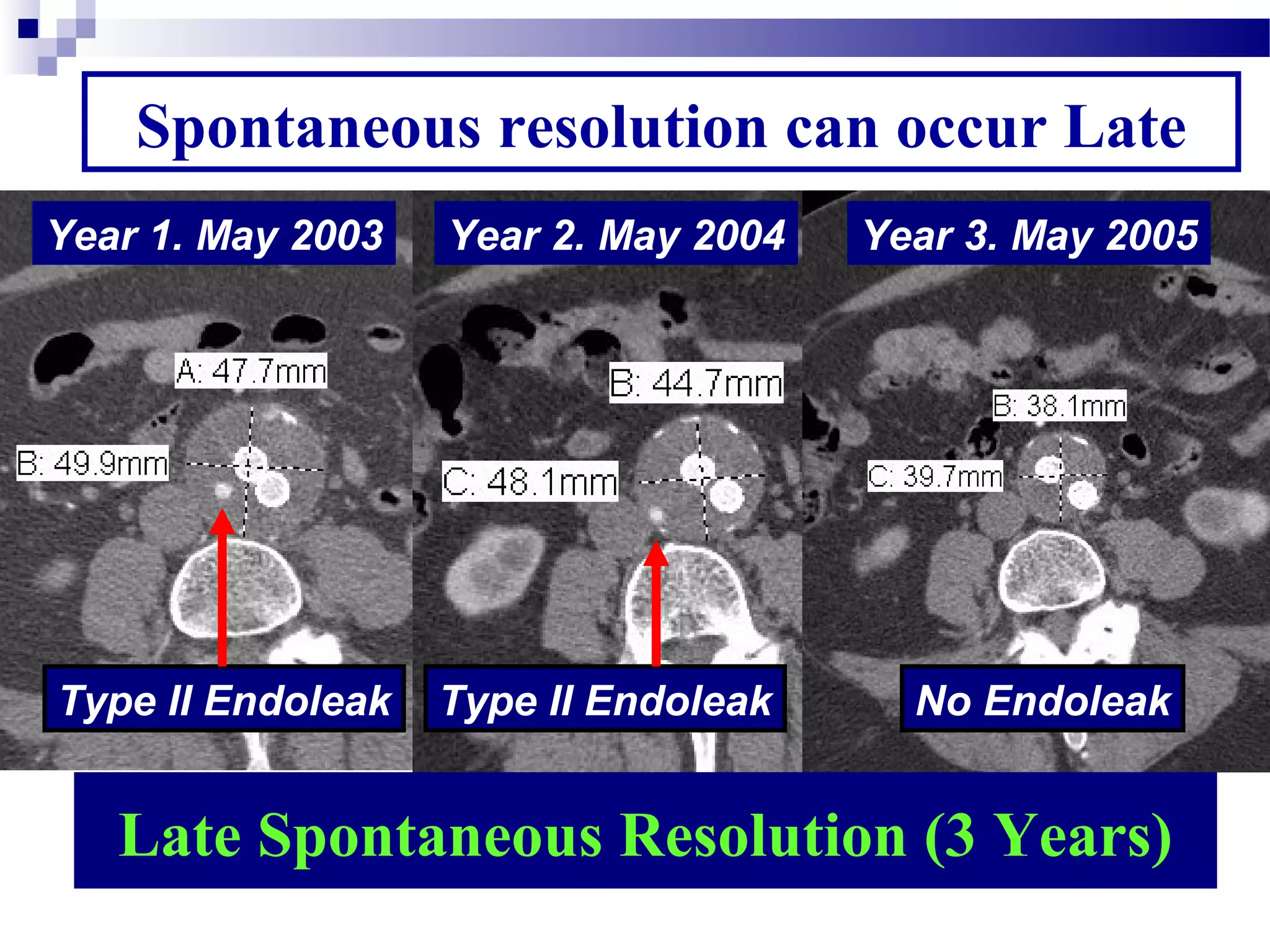
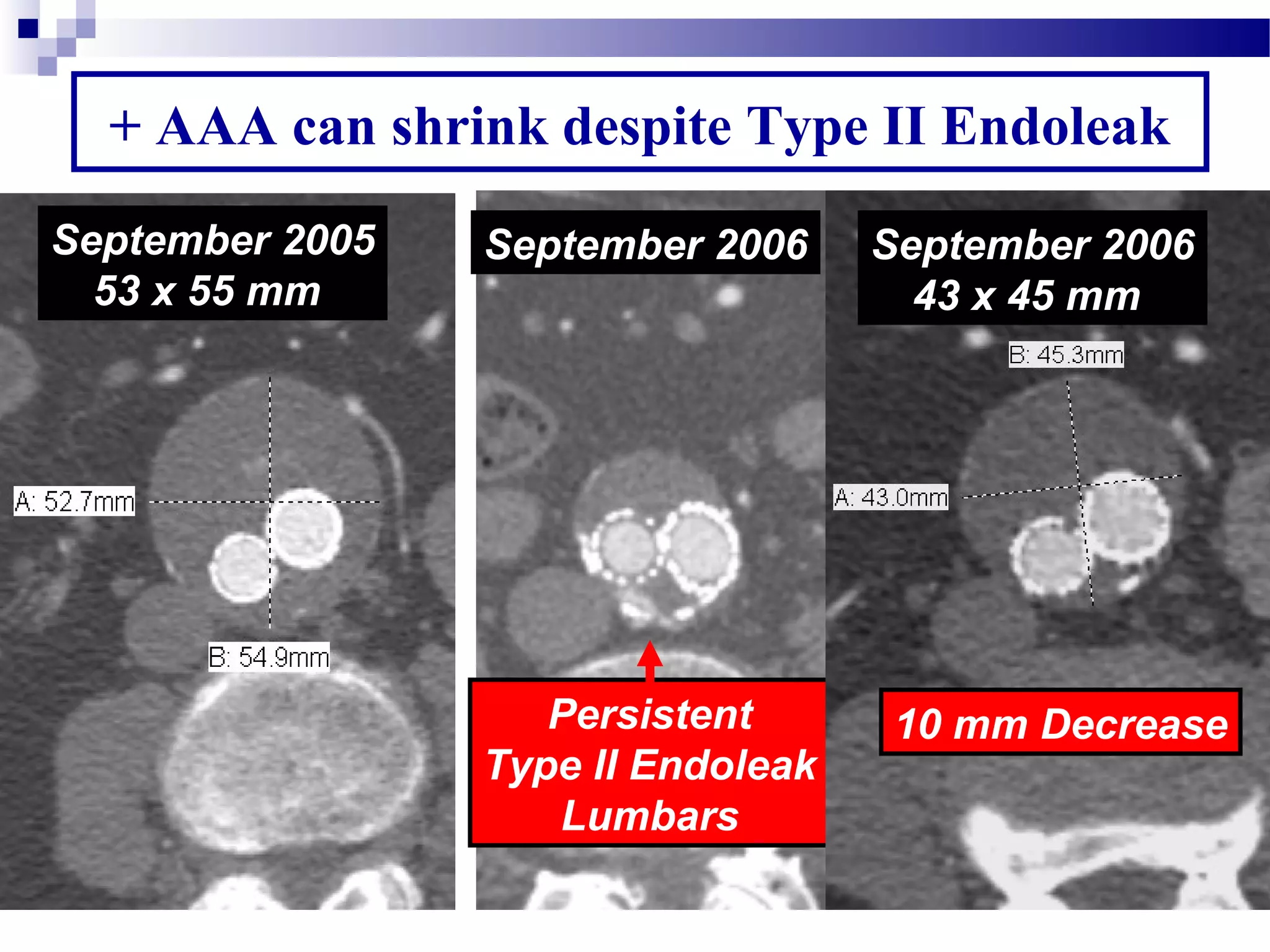
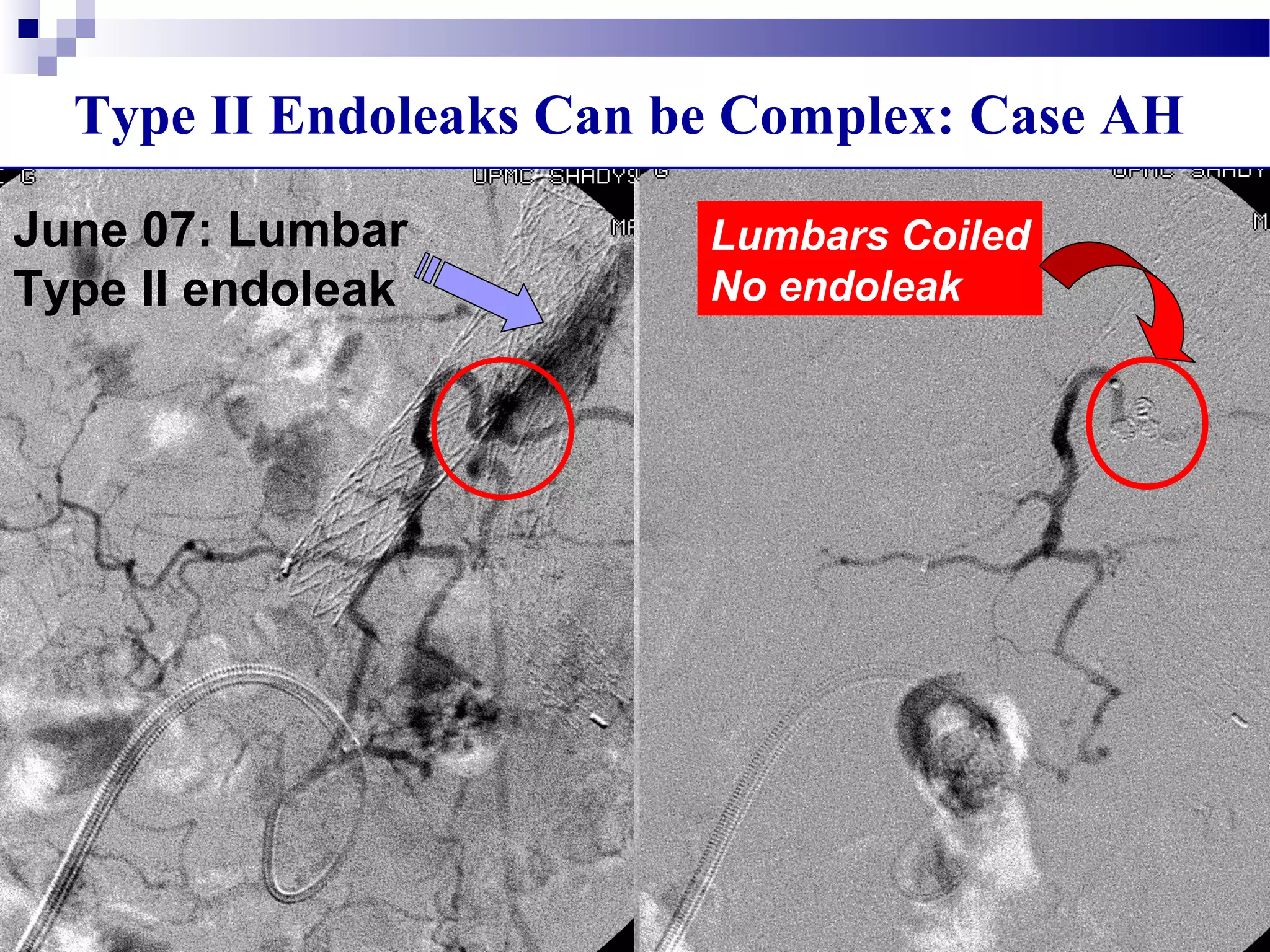
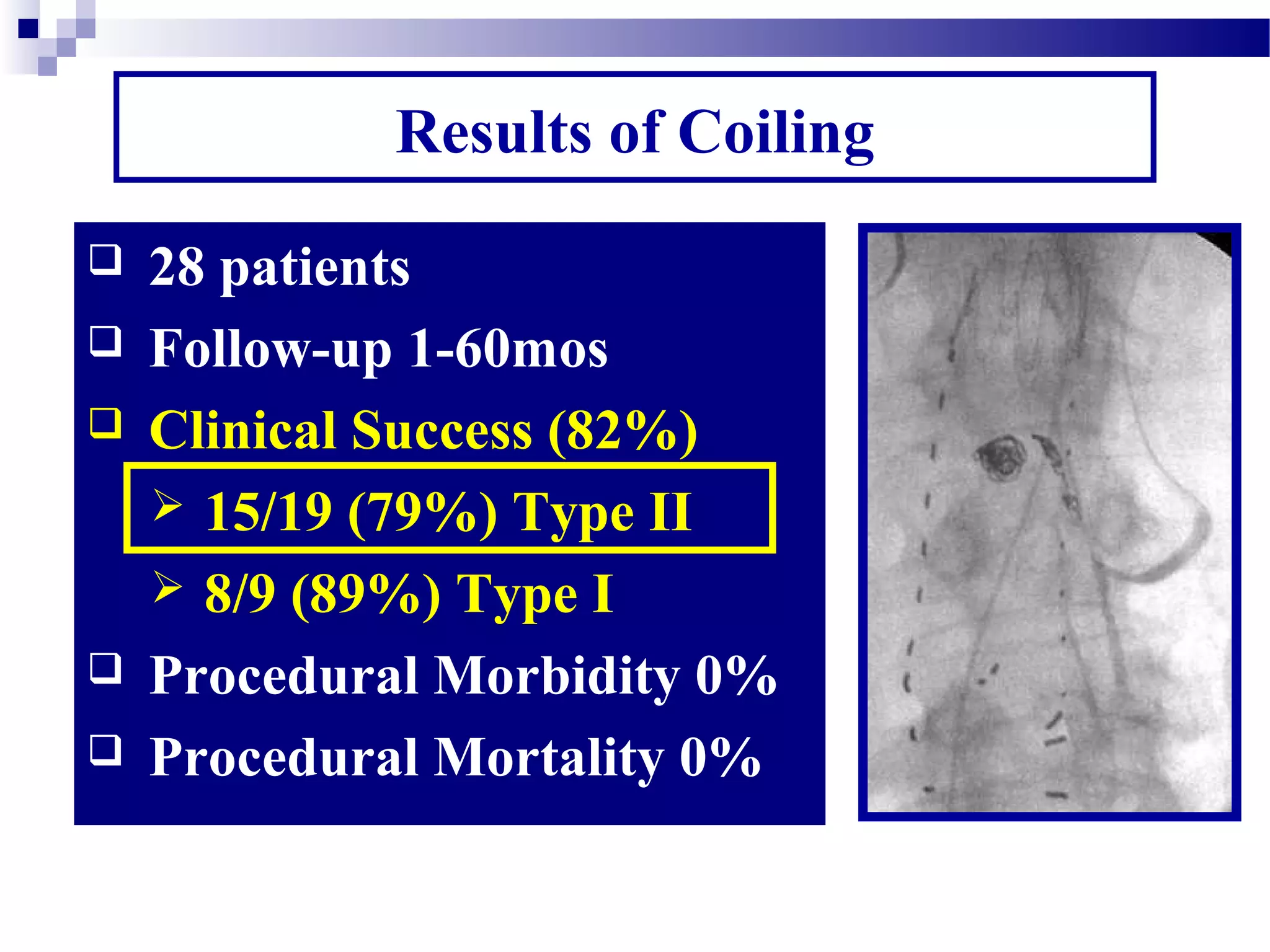
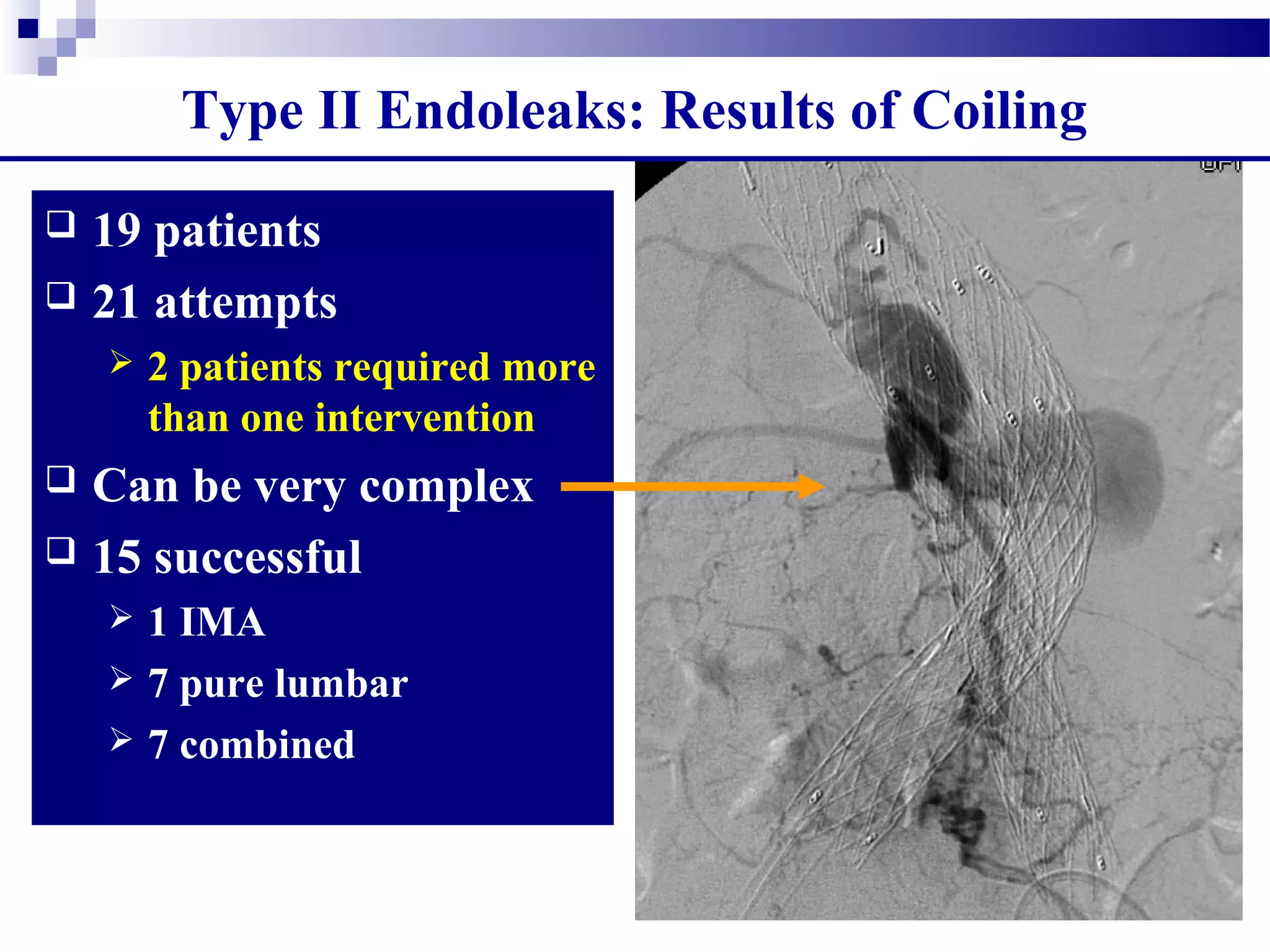
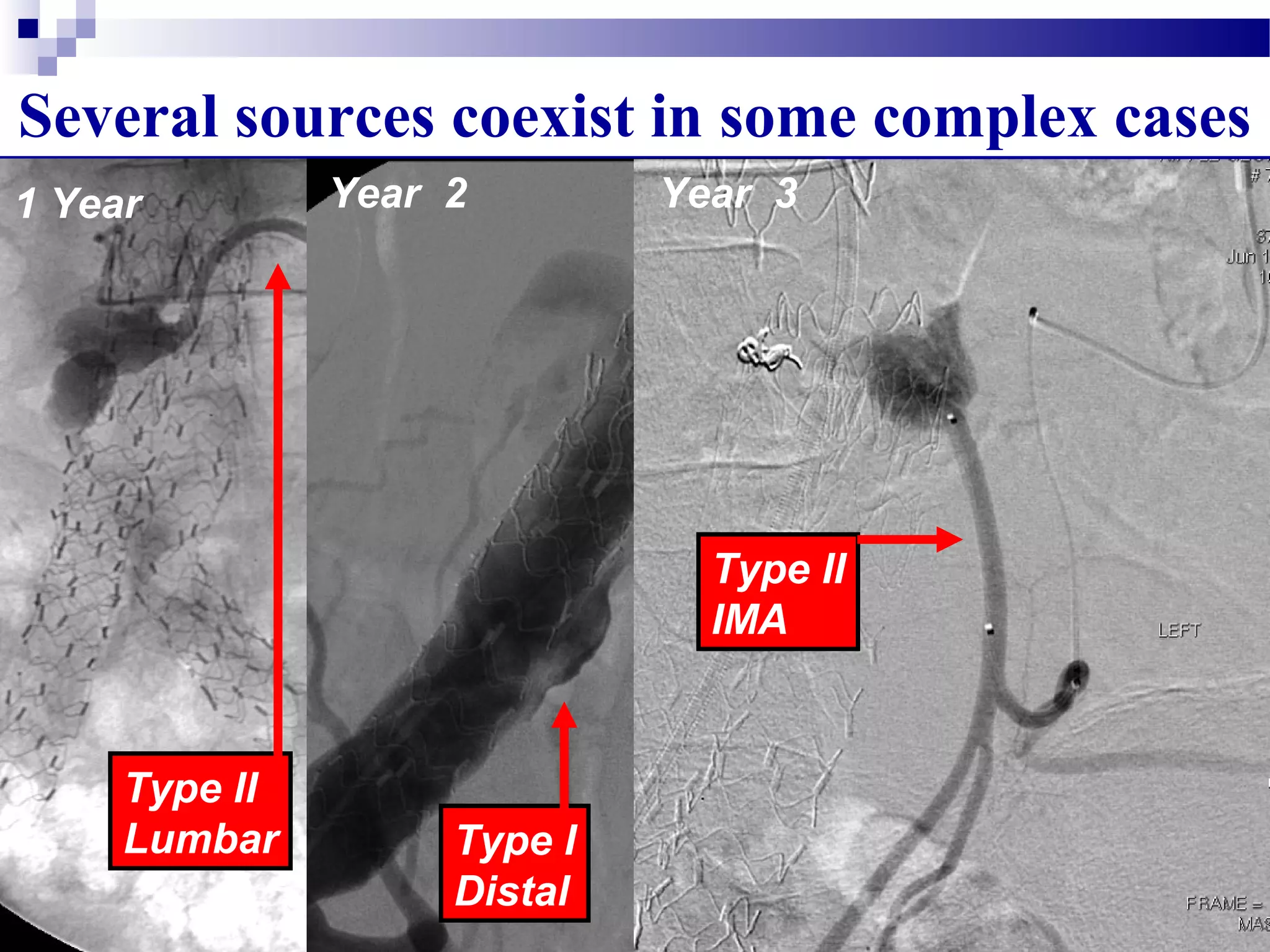
2. Type II endoleaks are more common but often have a benign natural history, with many resolving spontaneously. Treatment is only recommended if the aneurysm sac enlarges.
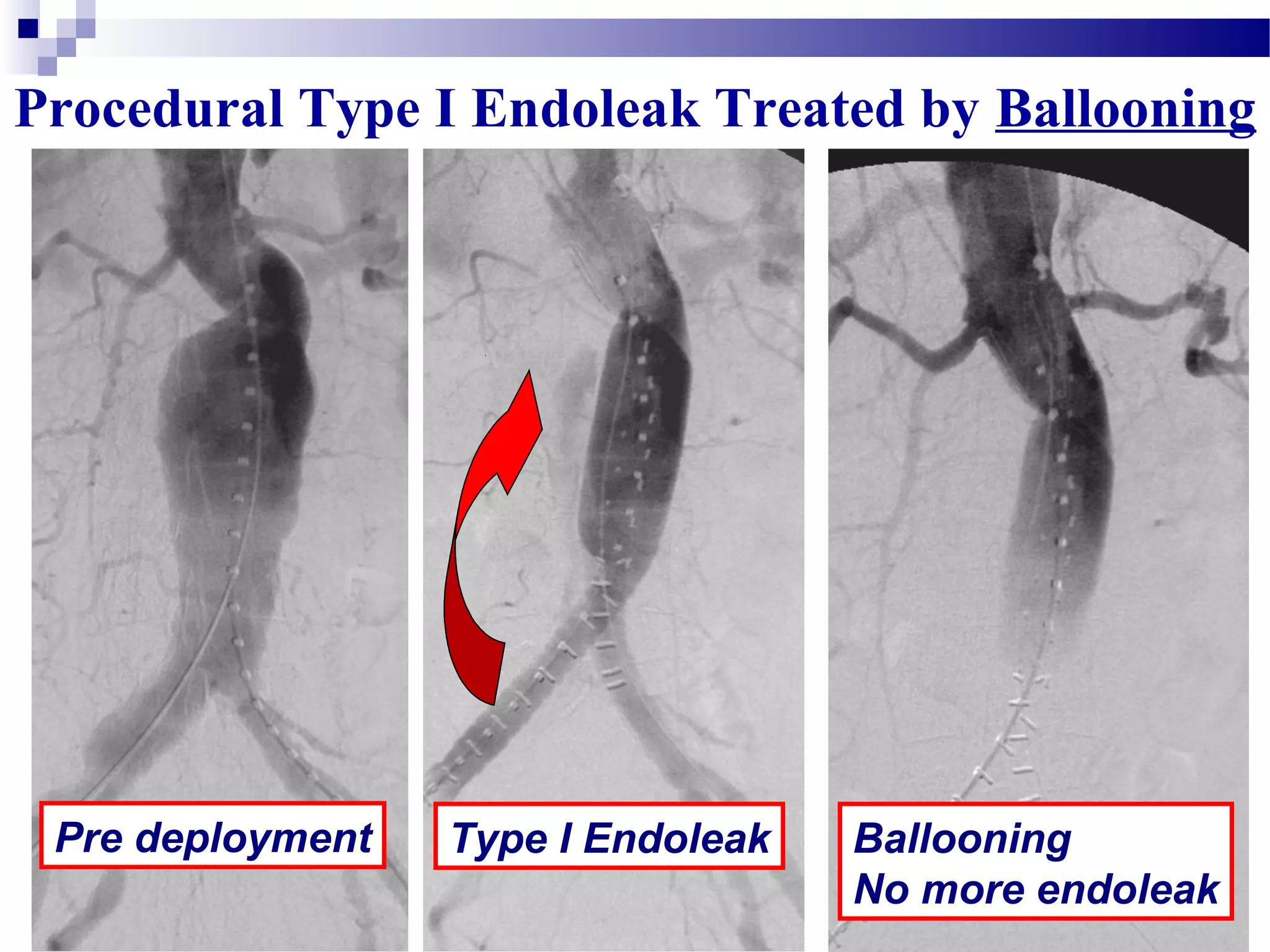
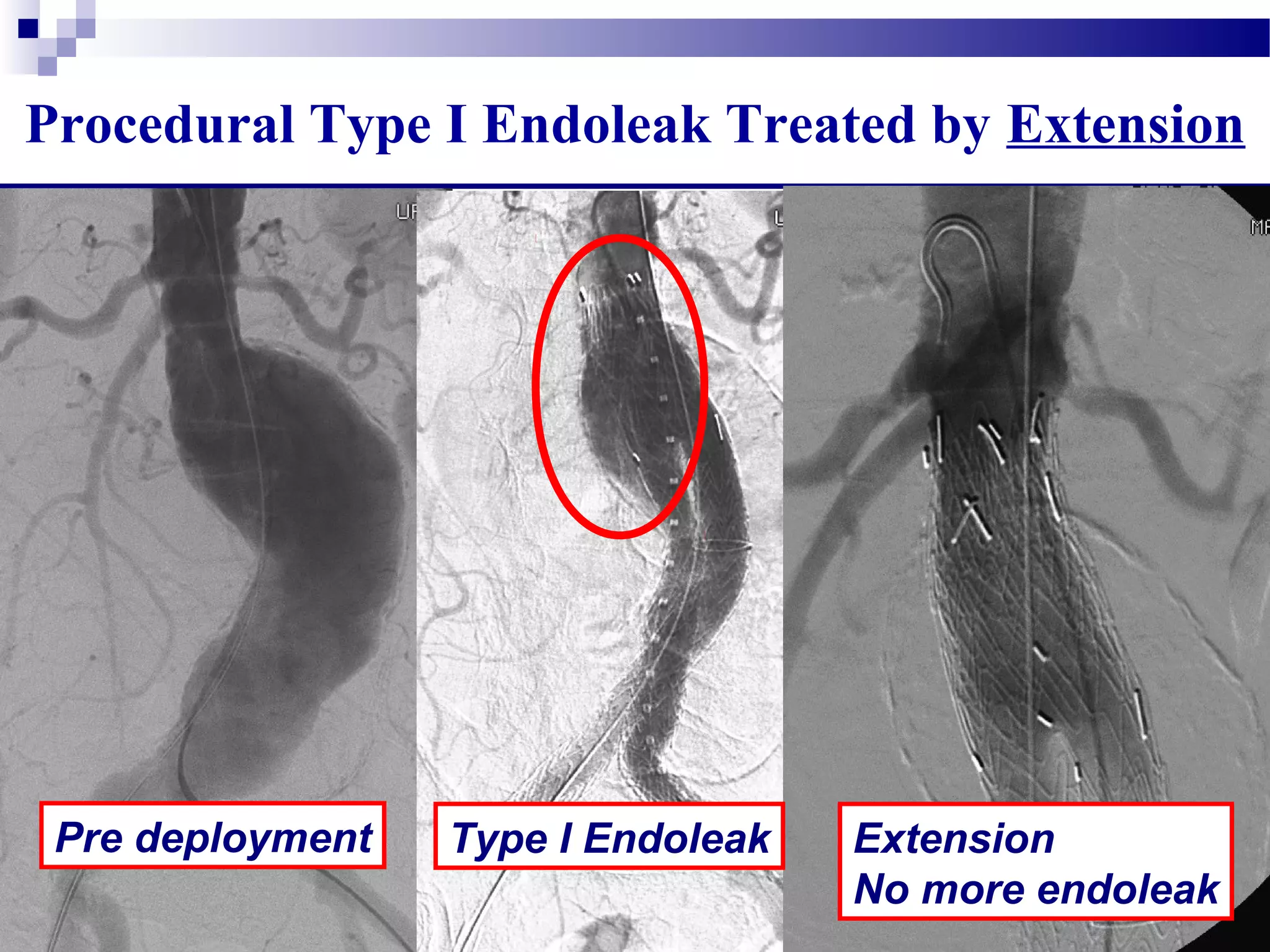
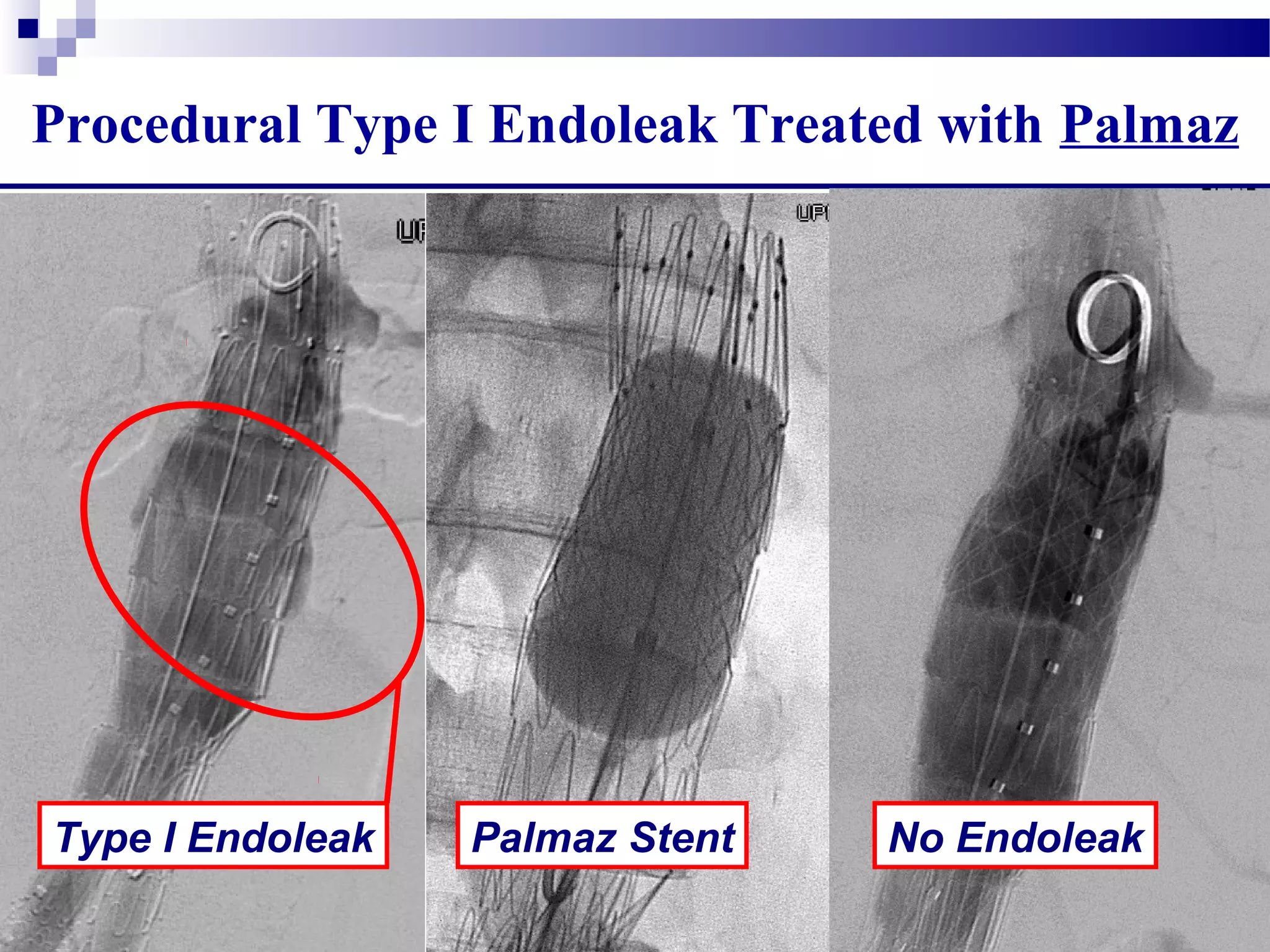
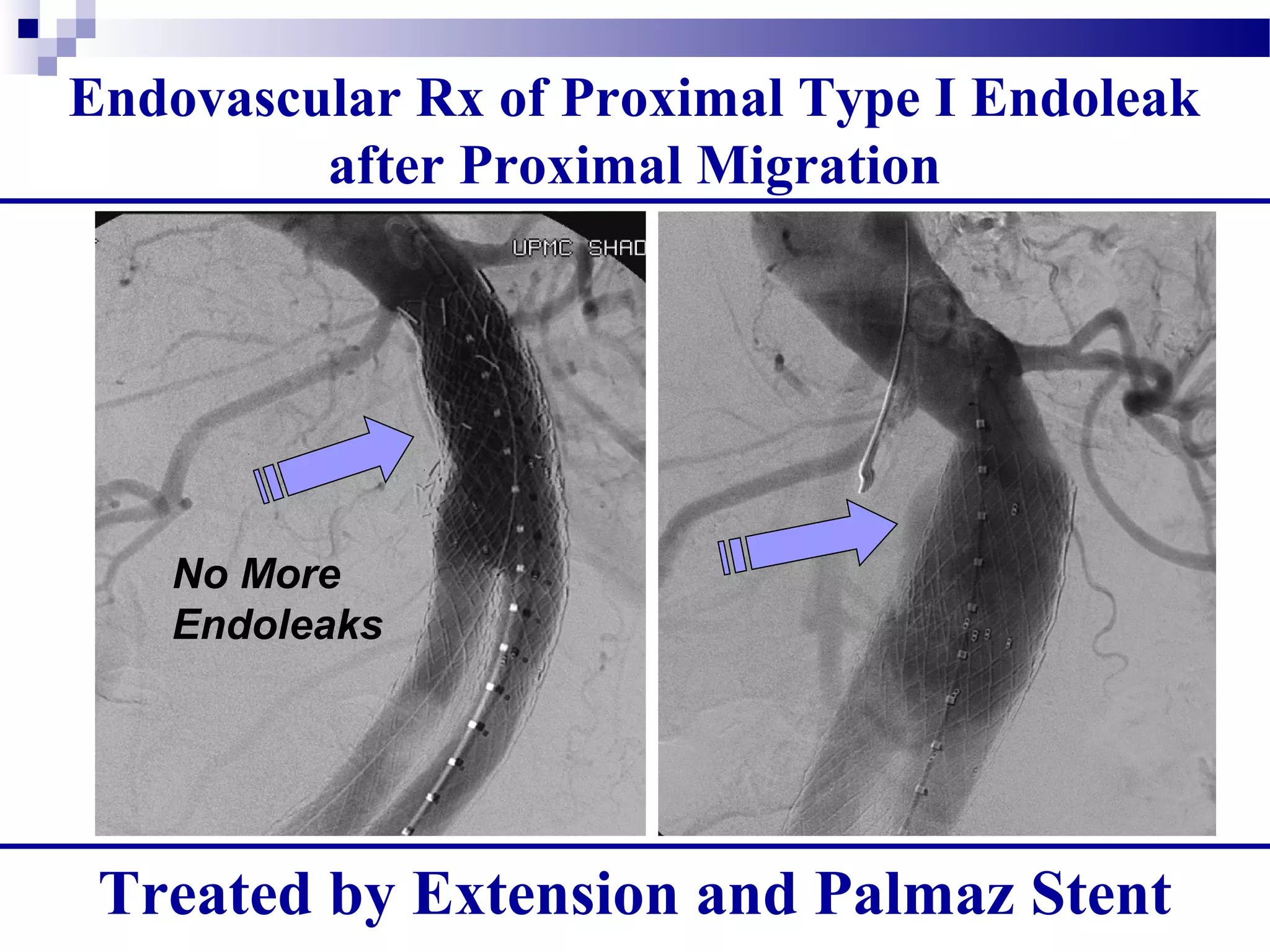
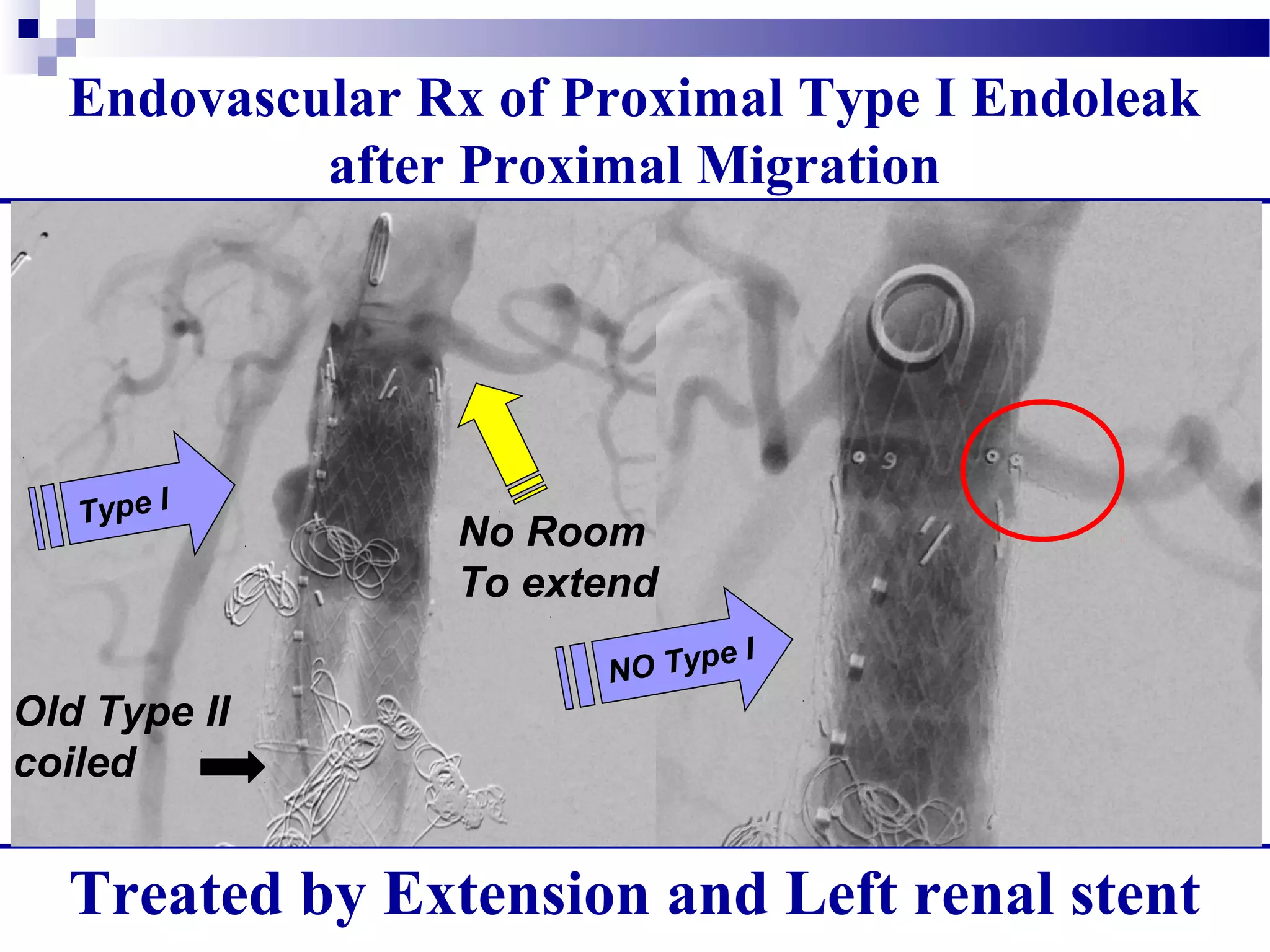
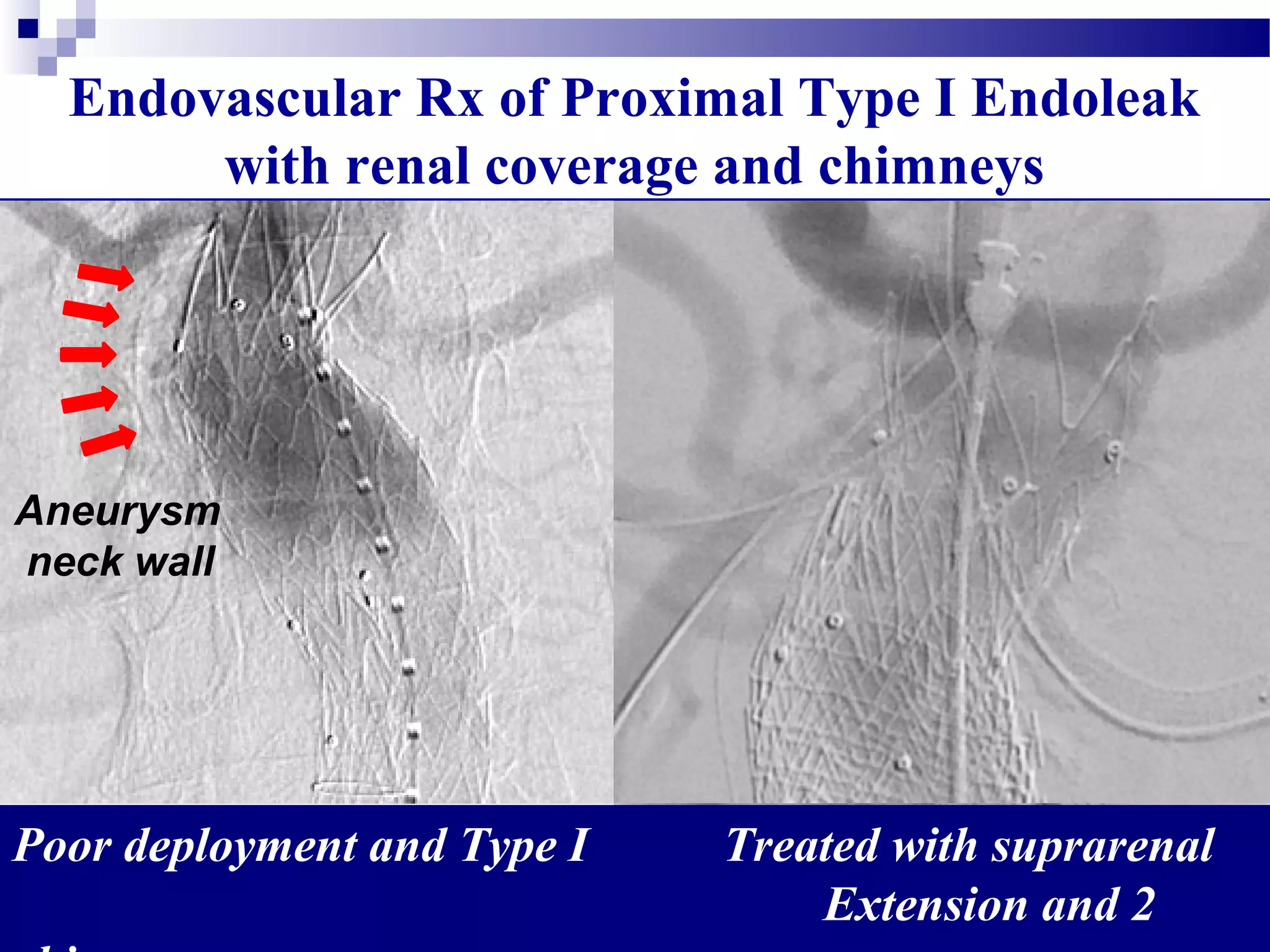
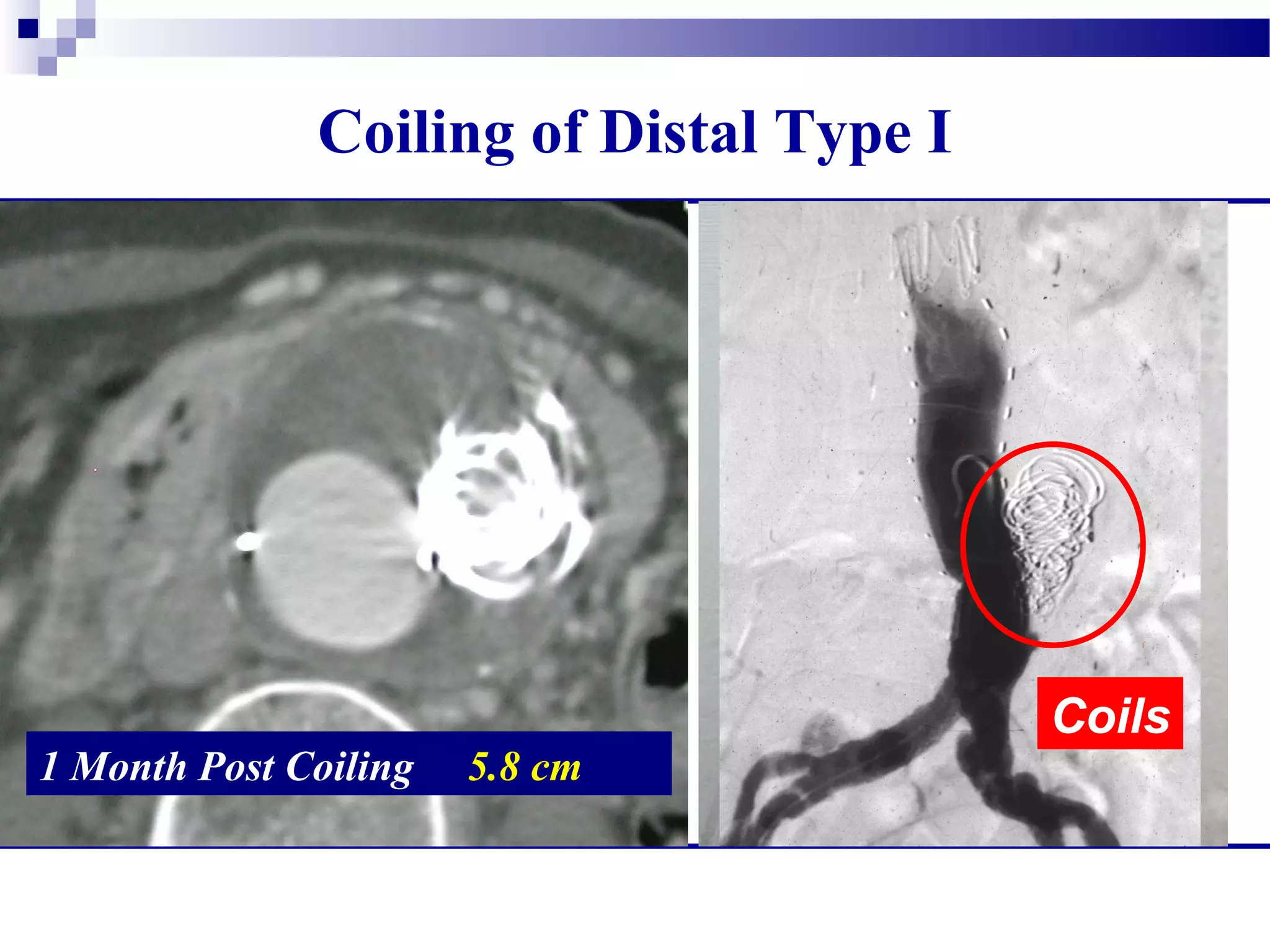
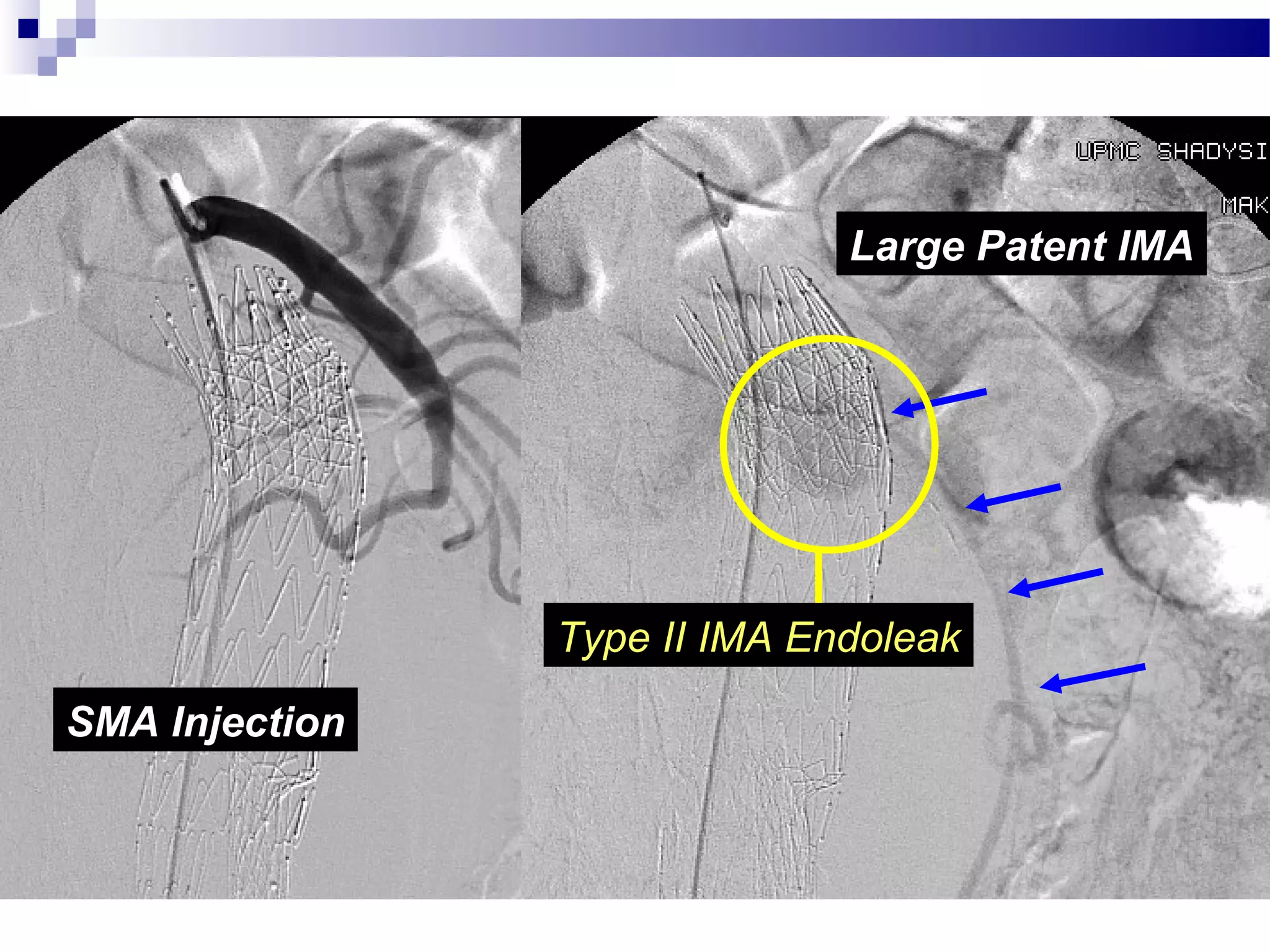
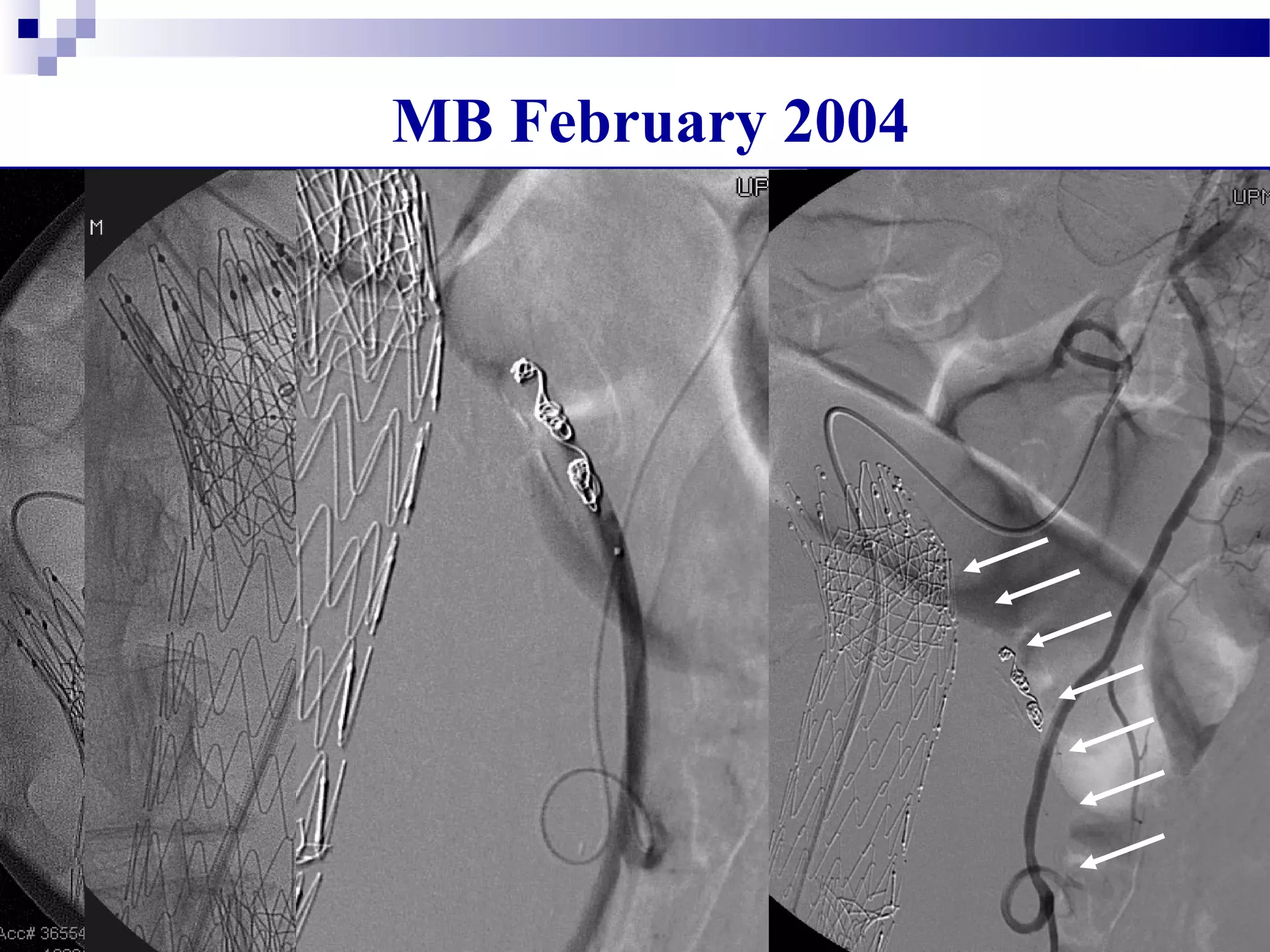
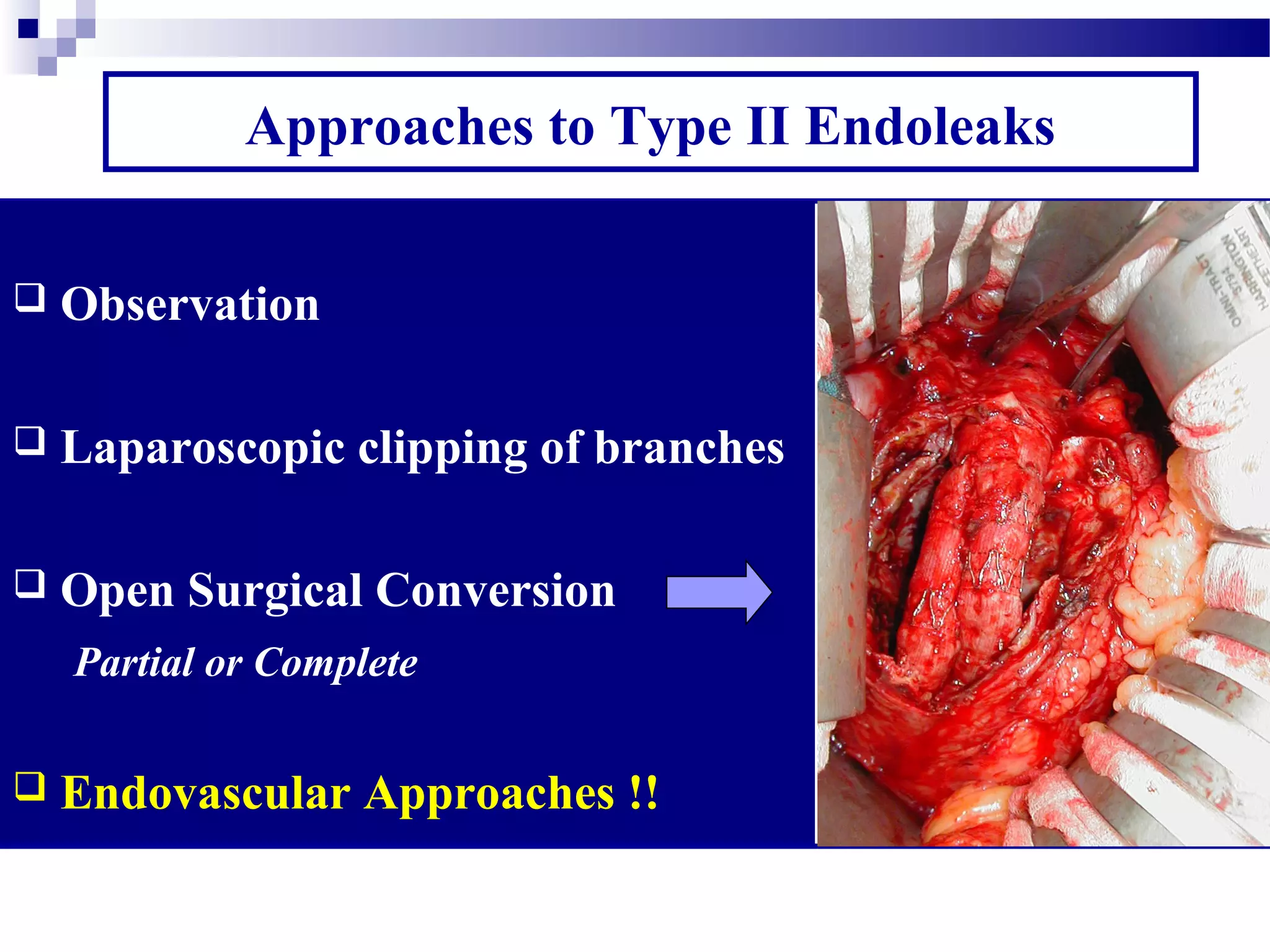
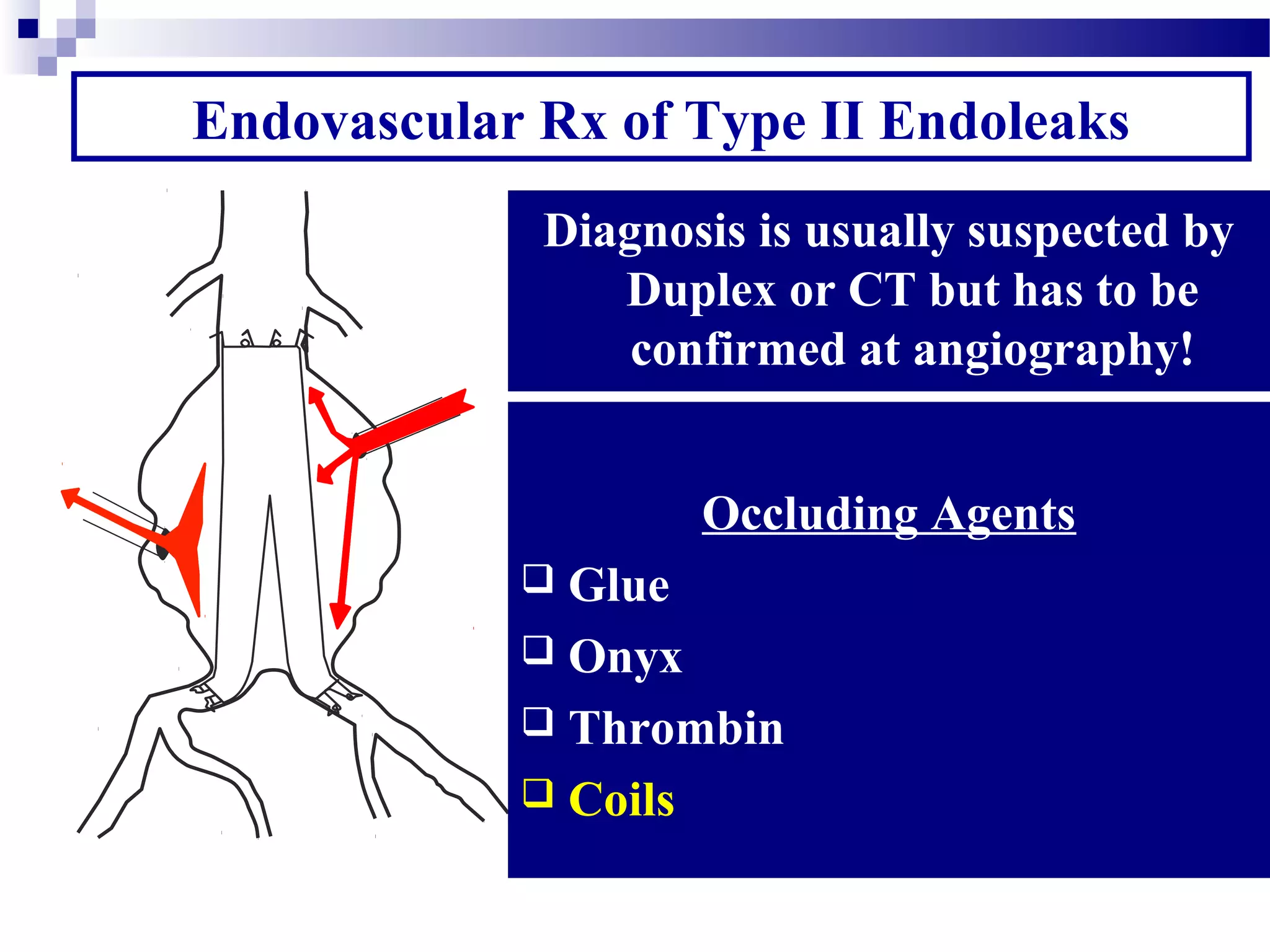
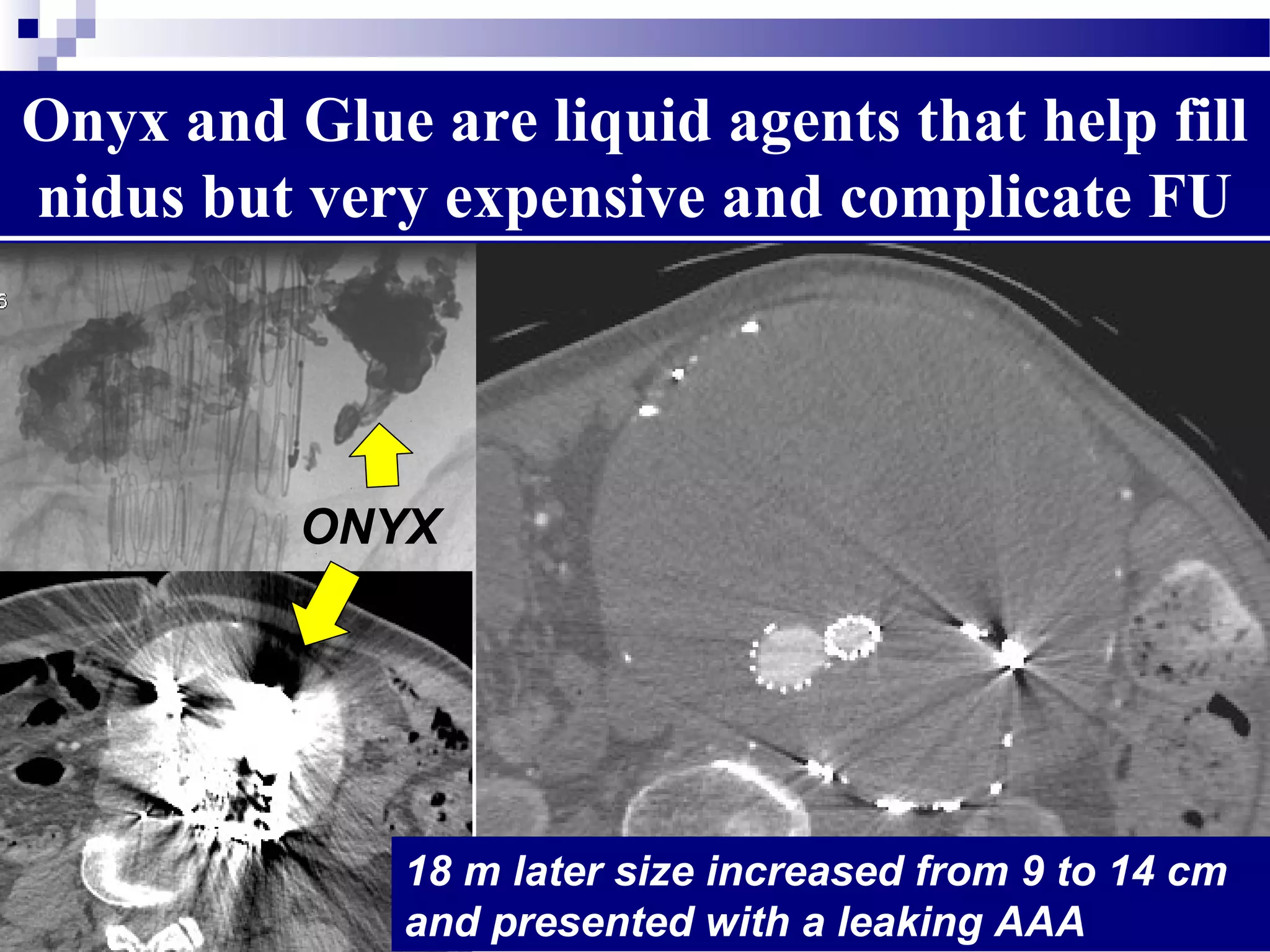
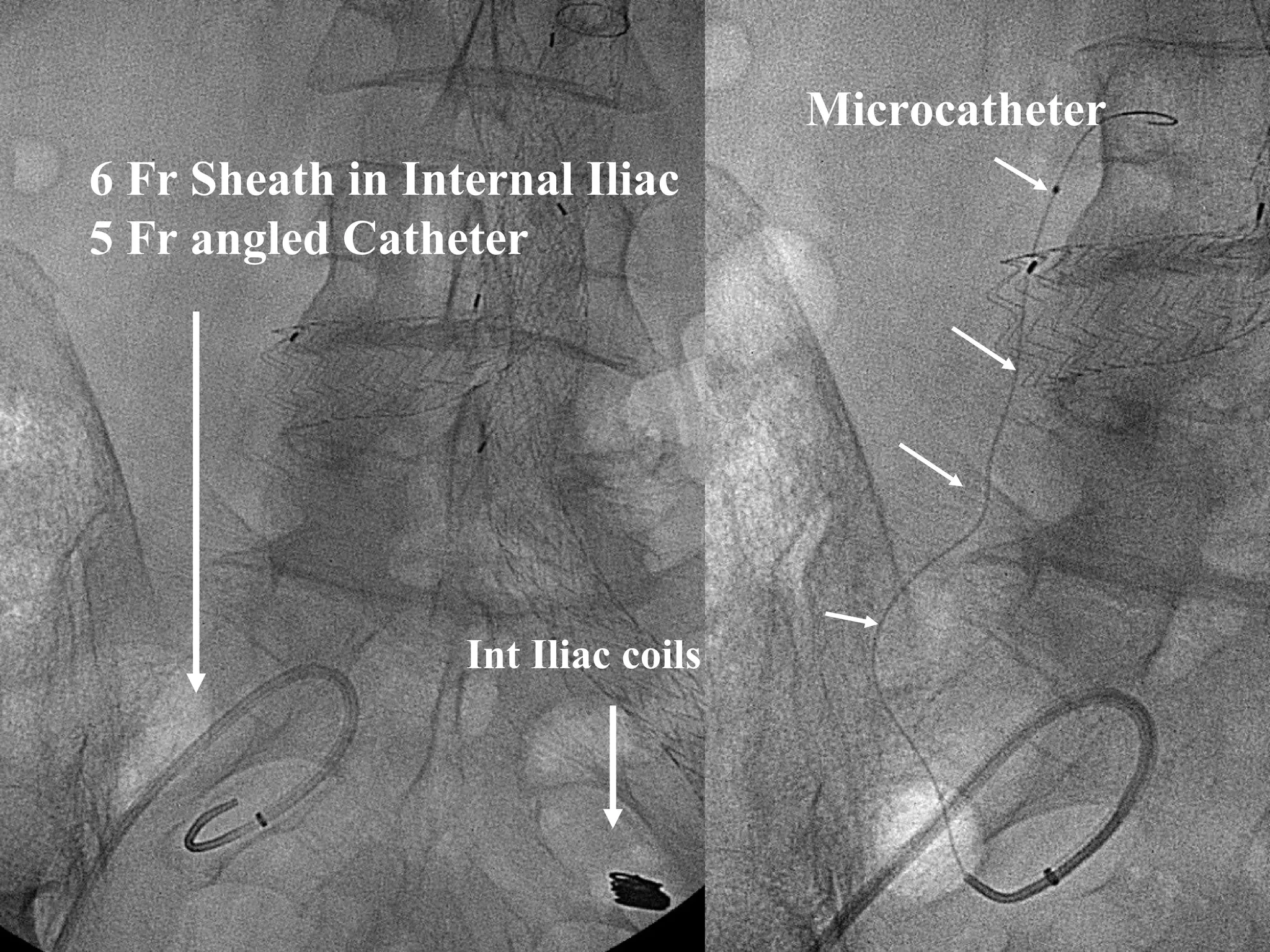
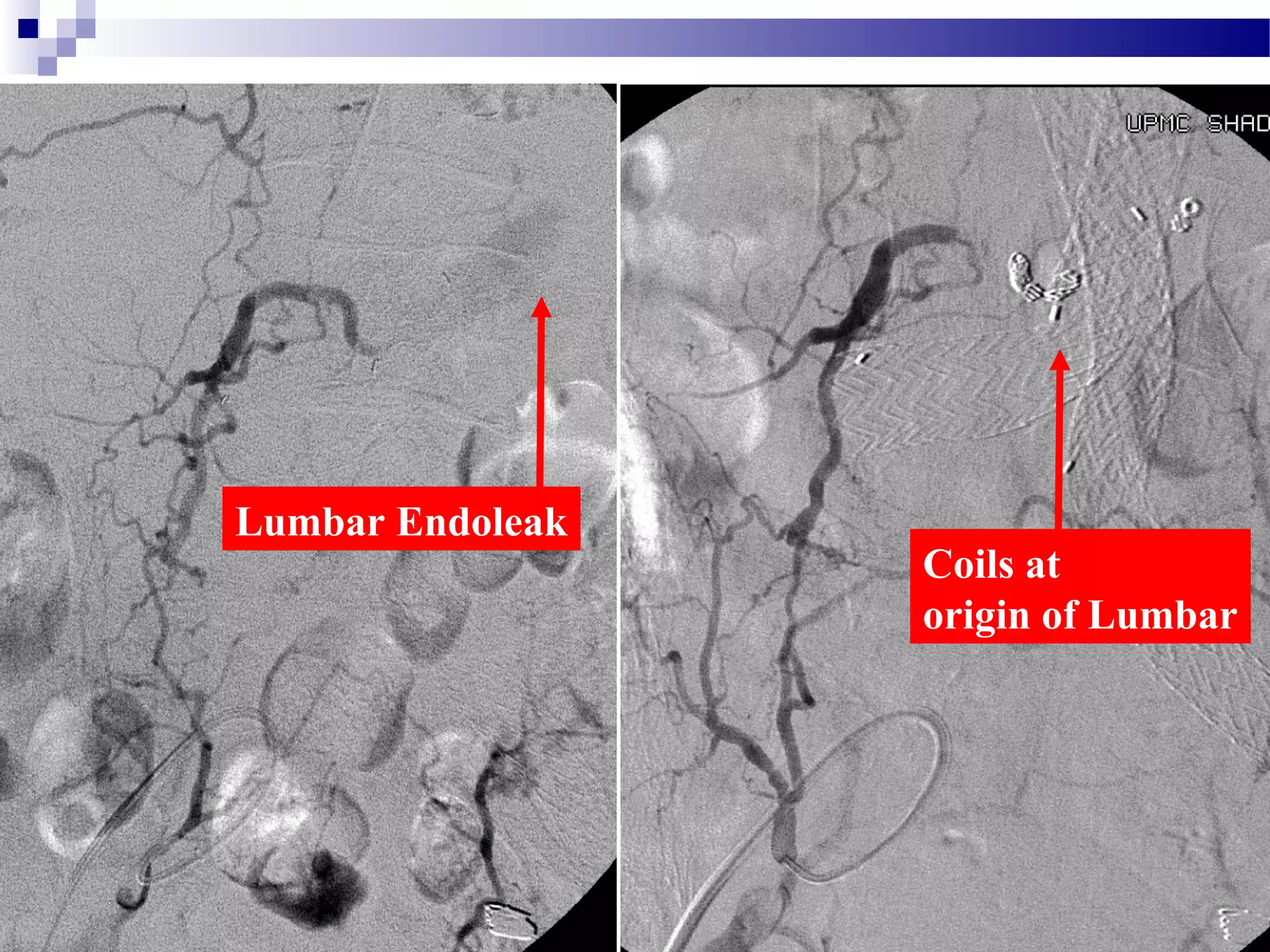
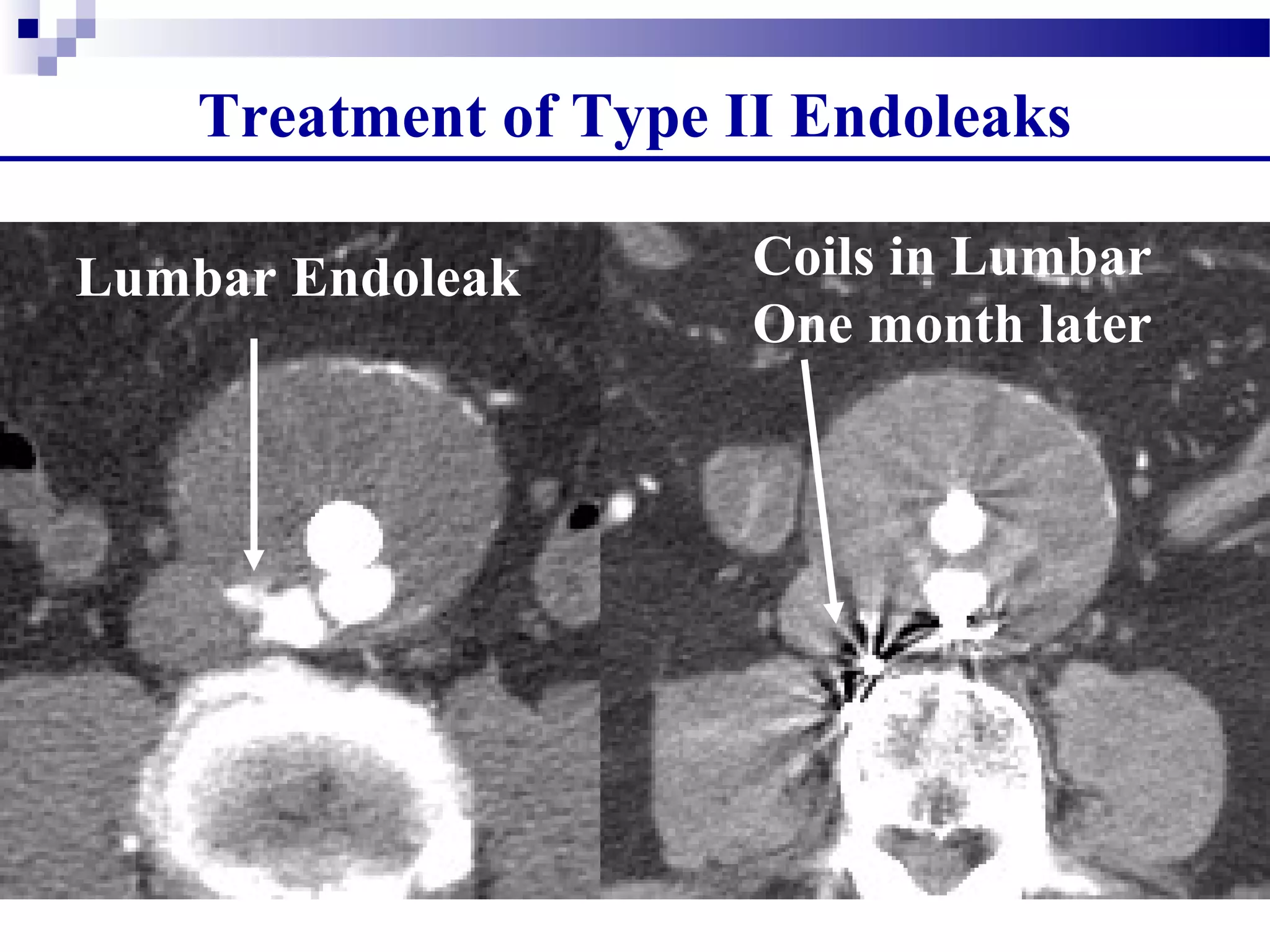
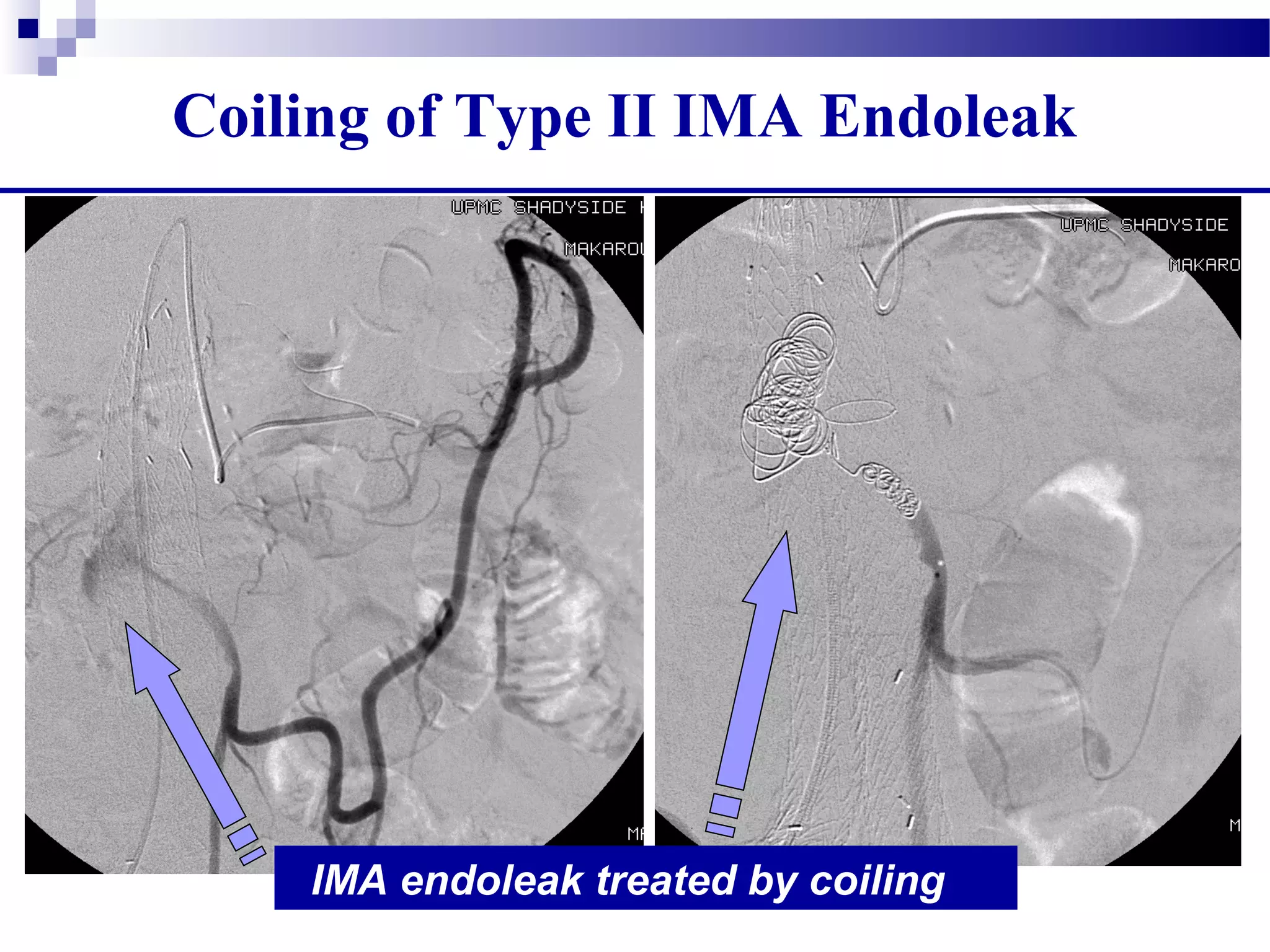
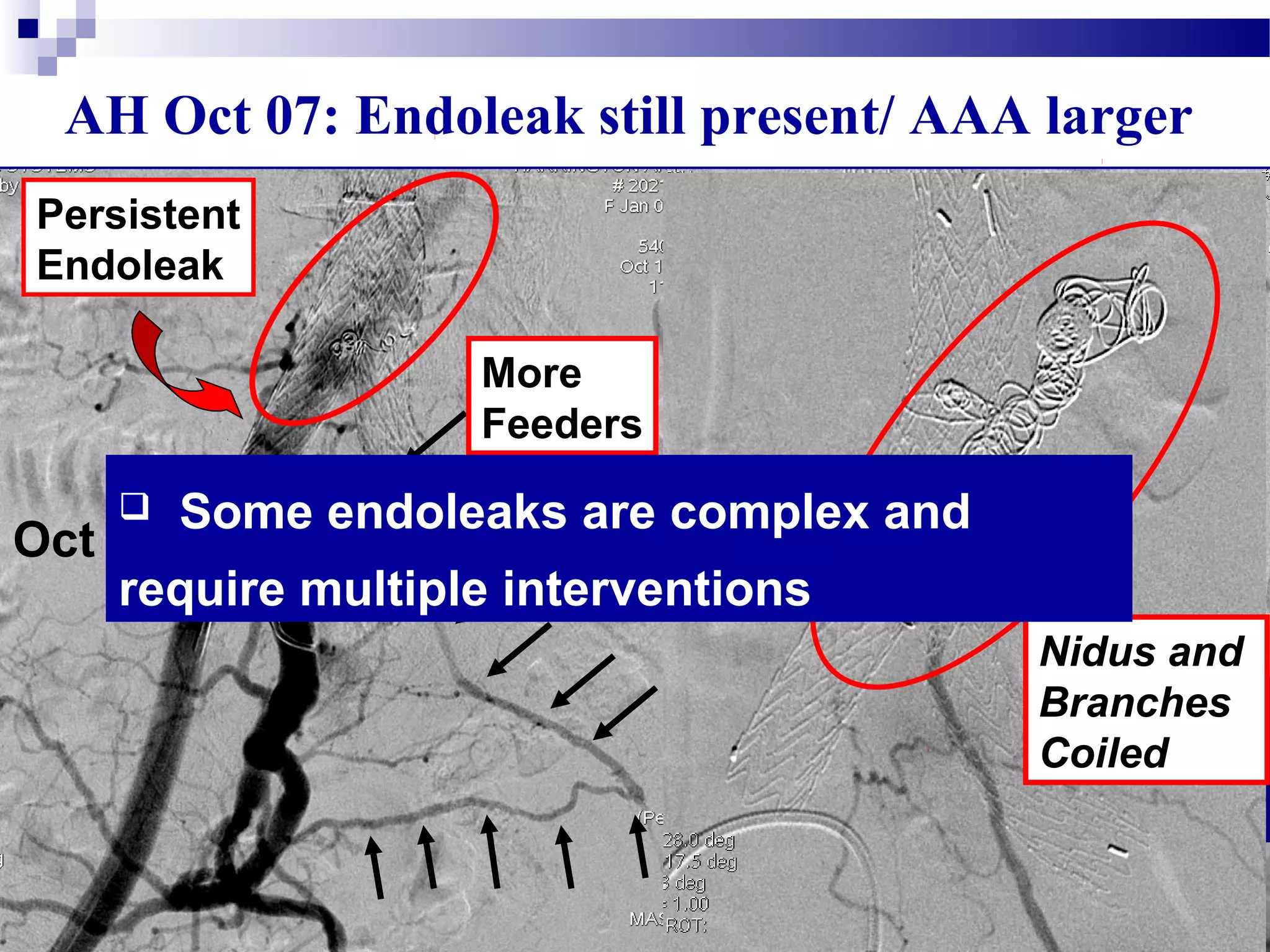
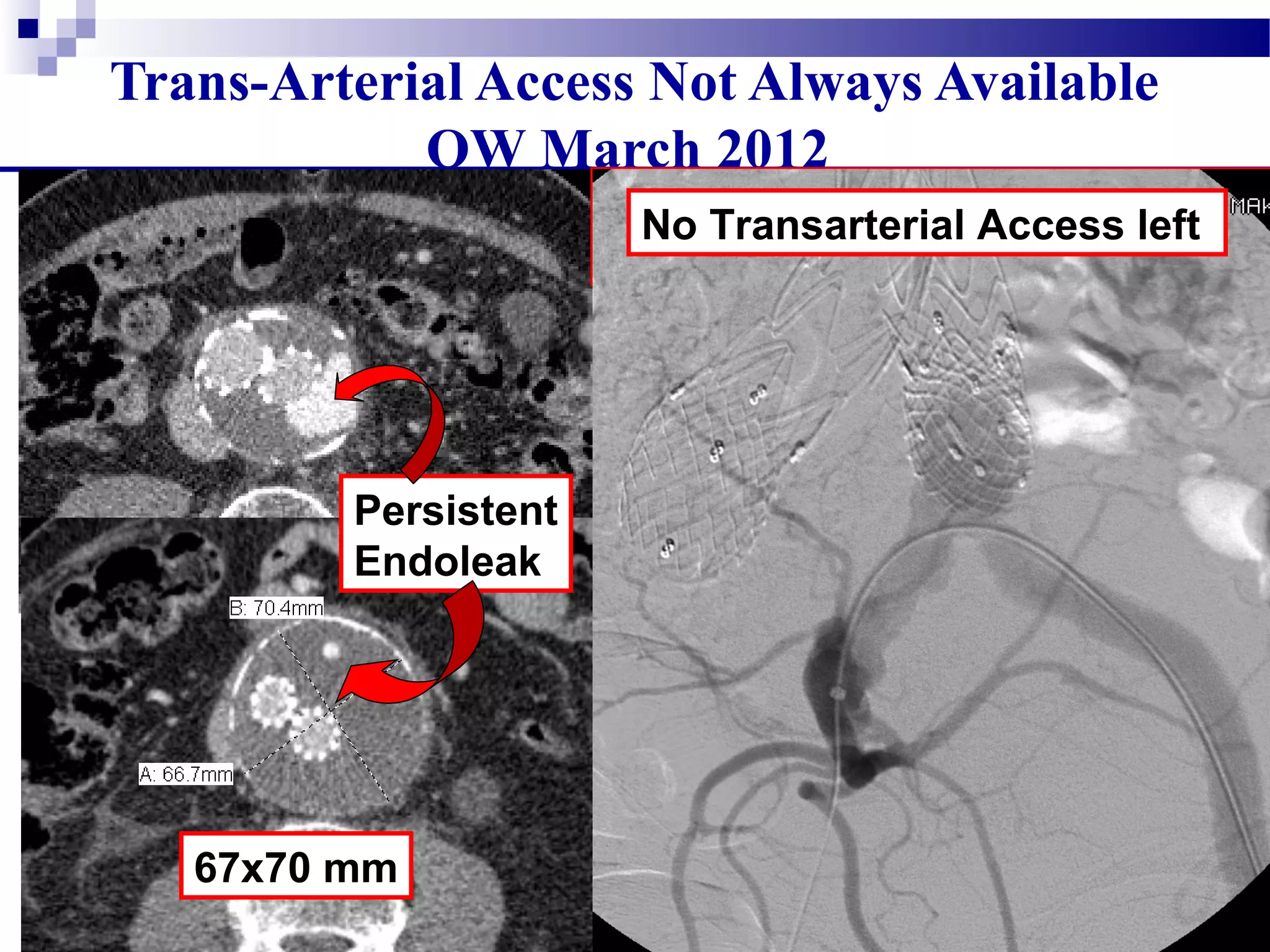
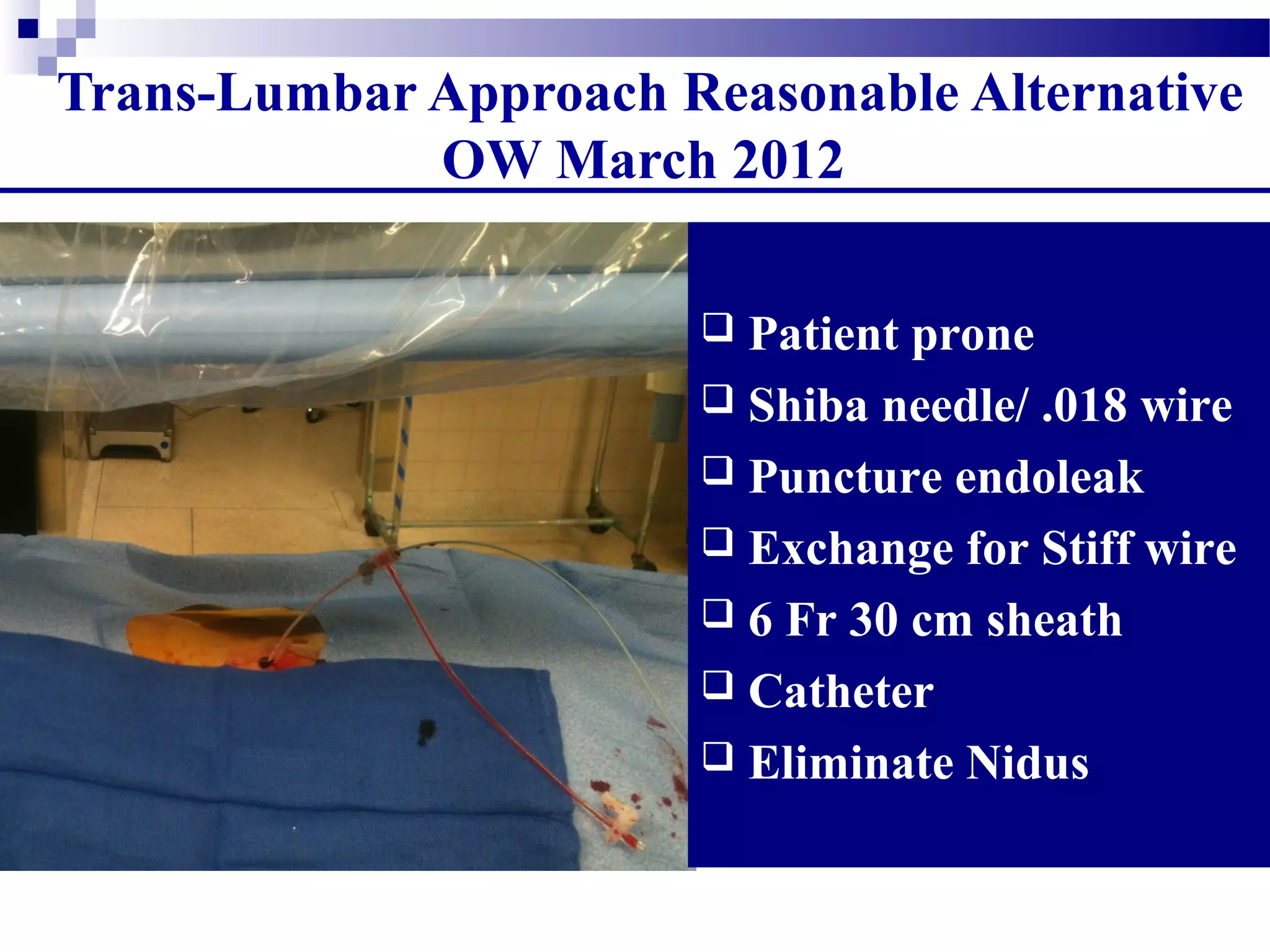
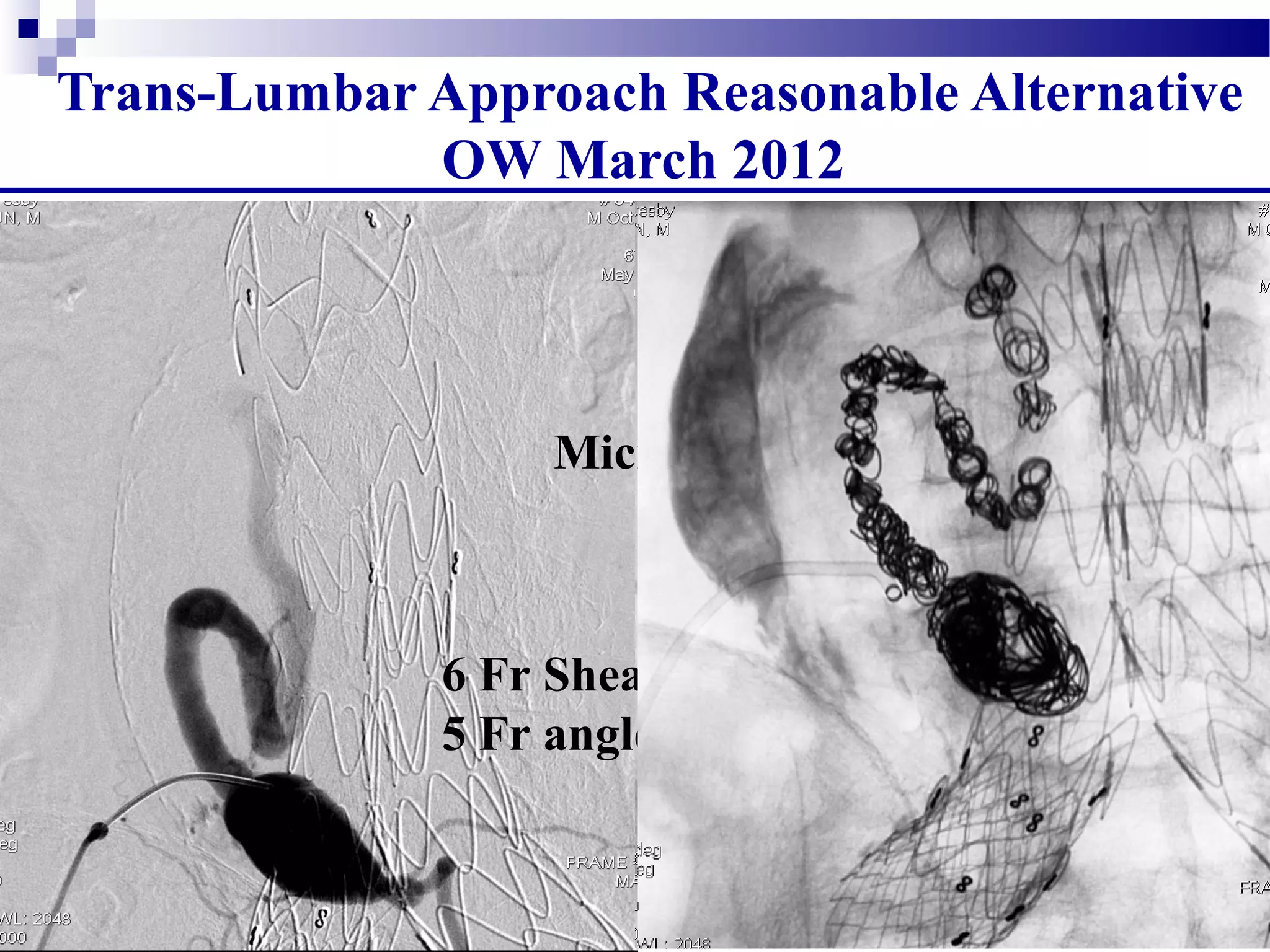
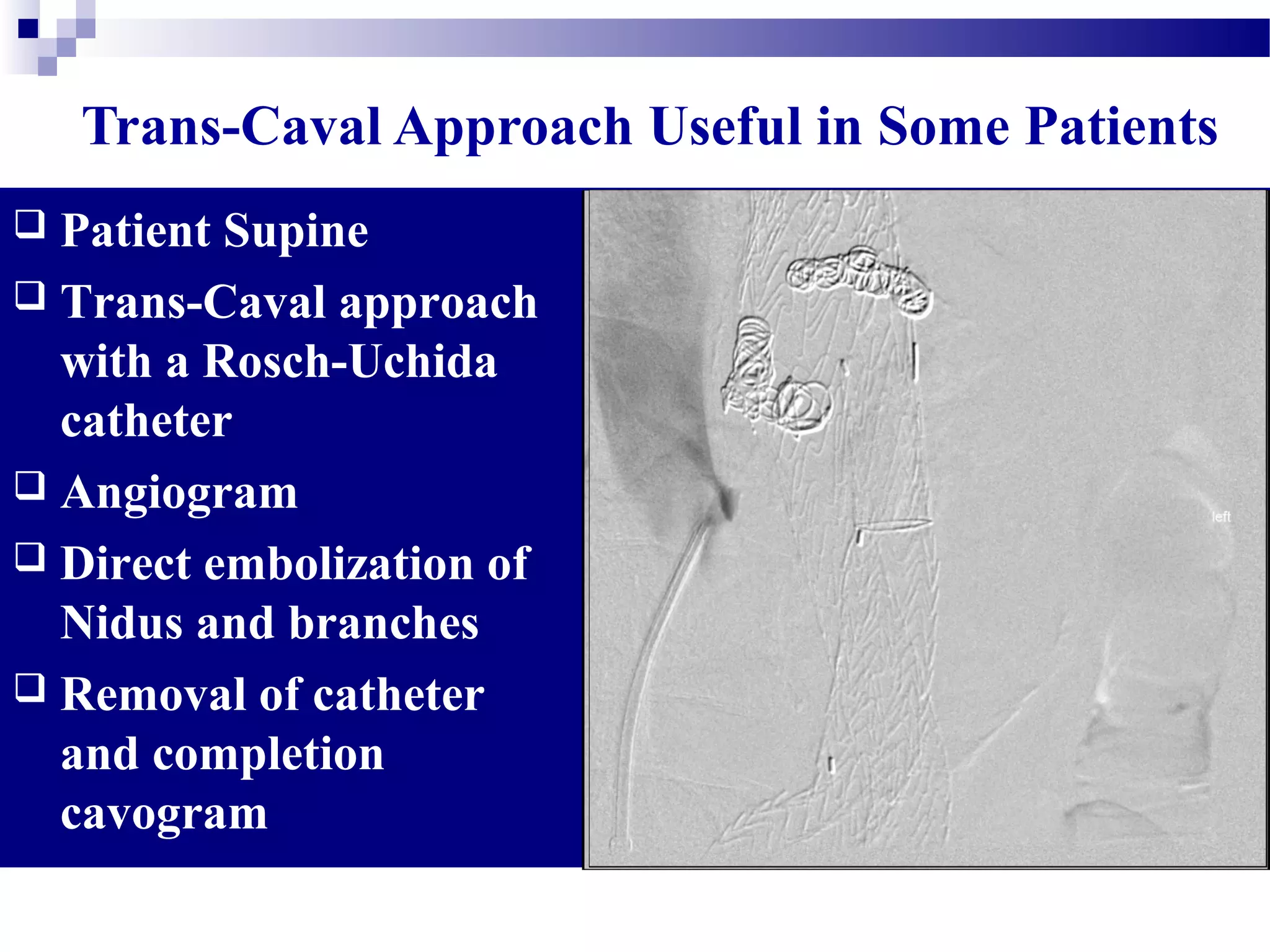
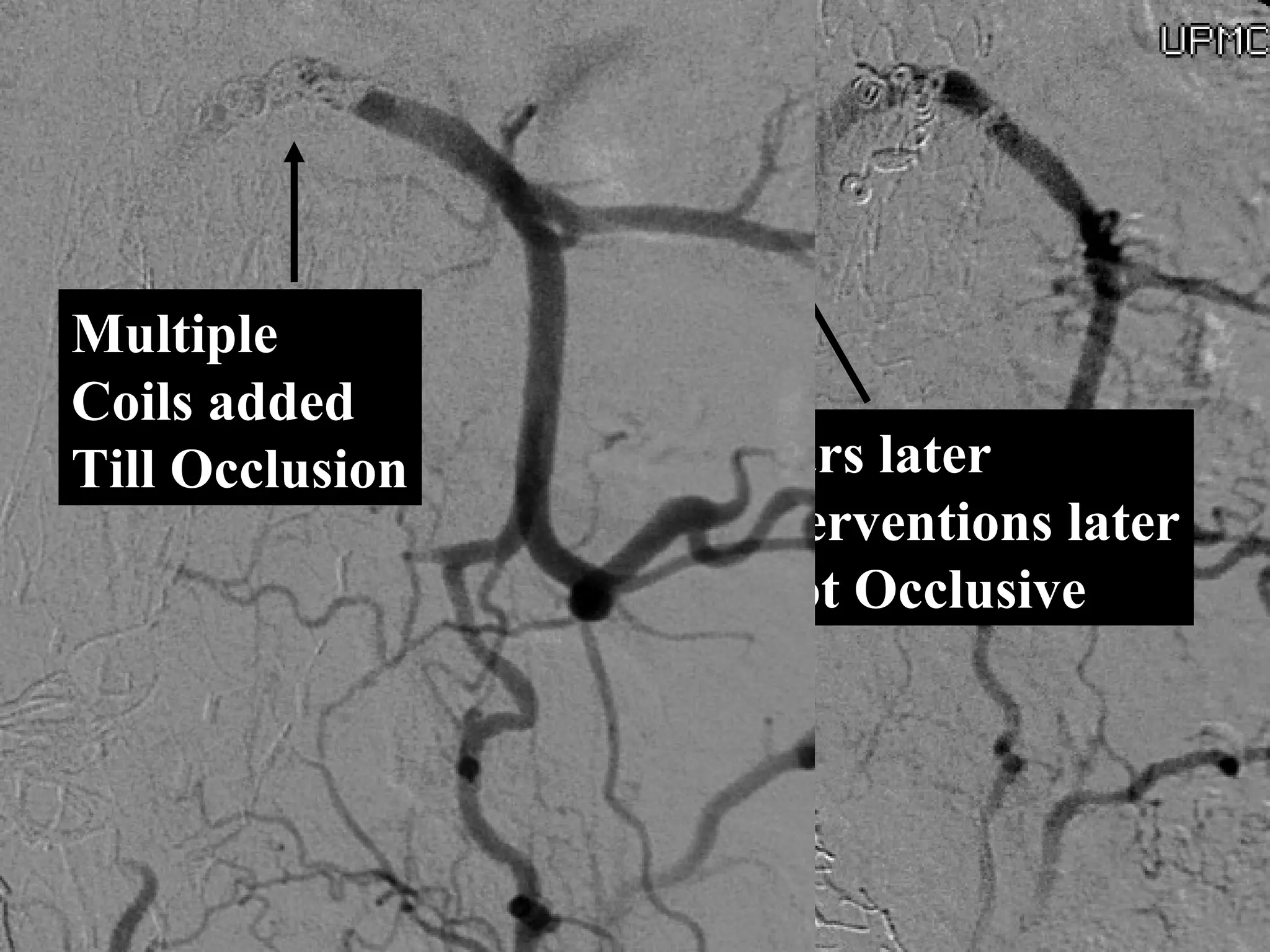
3. Endovascular techniques can be used to treat Type I, II, and III endoleaks via extensions, coils, glue, or onyx, with the goal of occluding the source of blood flow into the sac. Transarterial, translumbar, and transcaval approaches may be necessary depending on anatomy.