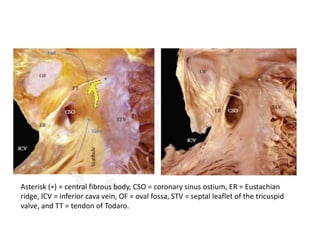
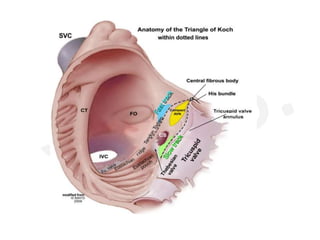
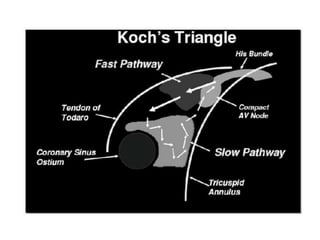
- Koch's triangle delineates the location of the atrioventricular node. It is bounded posteriorly by the tendon of Todaro, anteriorly by the tricuspid valve septal leaflet, and inferiorly by the coronary sinus ostium.
- The atrioventricular node and His bundle are located near the apex of the triangle where the His bundle penetrates the central fibrous body. Catheter ablation for atrioventrial nodal reentrant tachycardia often targets the slow pathway region within the triangle.
- The dimensions and structures within Koch's triangle can vary between individuals, which is clinically relevant for catheter ablation procedures guided by anatomic landmarks in this region.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







