This document discusses gastrointestinal bleeding, including:
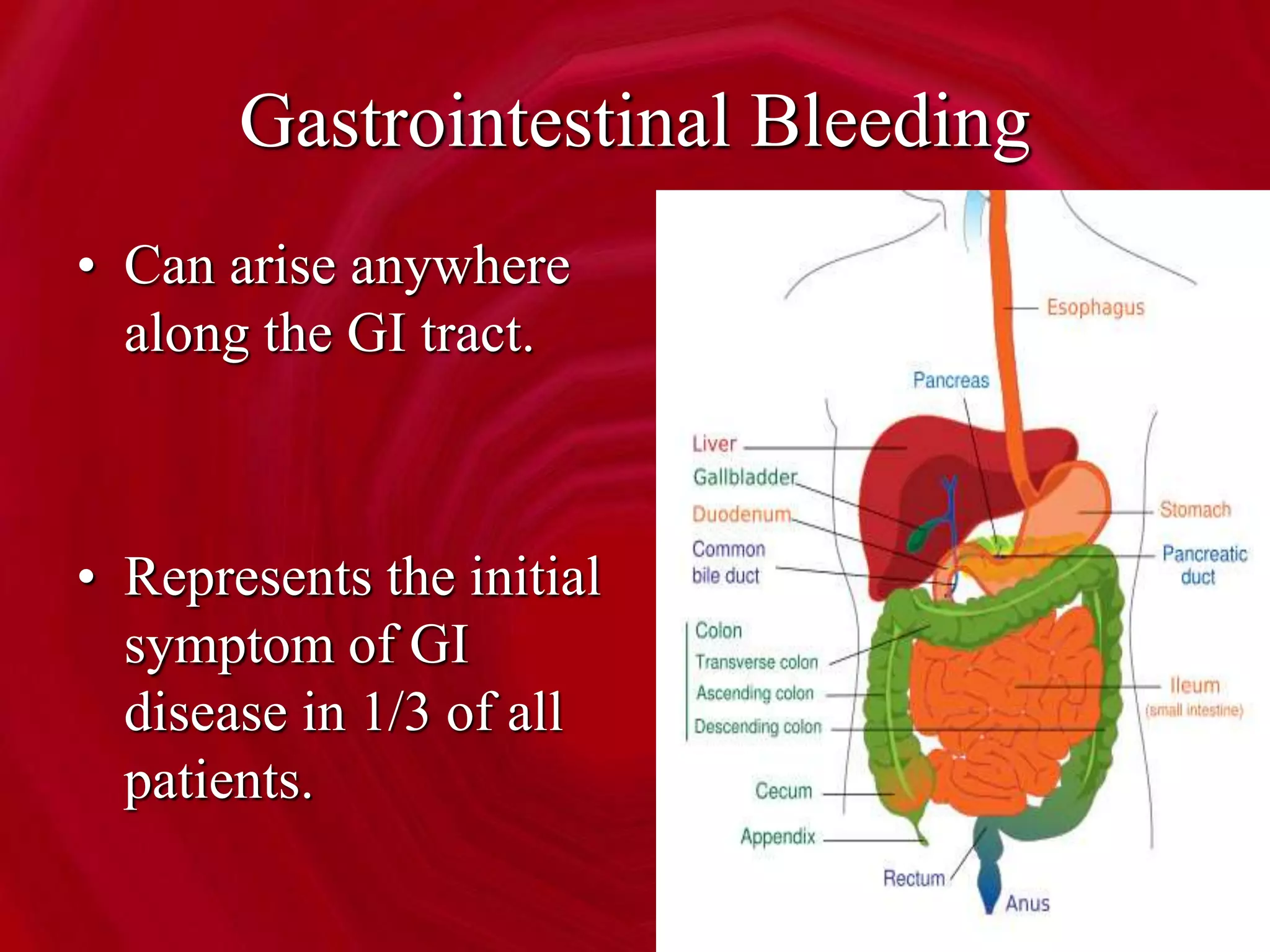
- Gastrointestinal bleeding can arise from any location in the GI tract and represents the initial symptom of GI disease in 1/3 of patients.
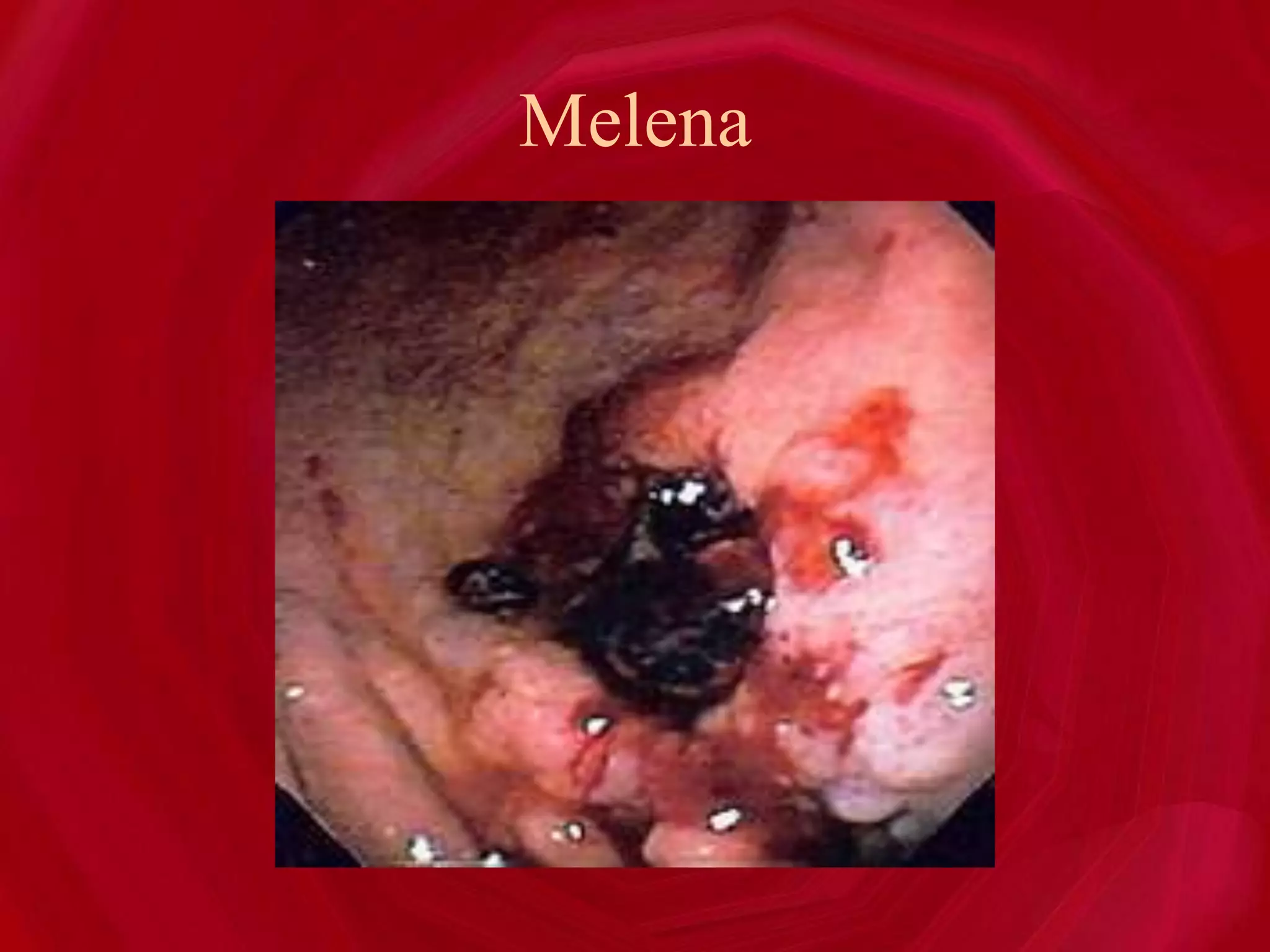
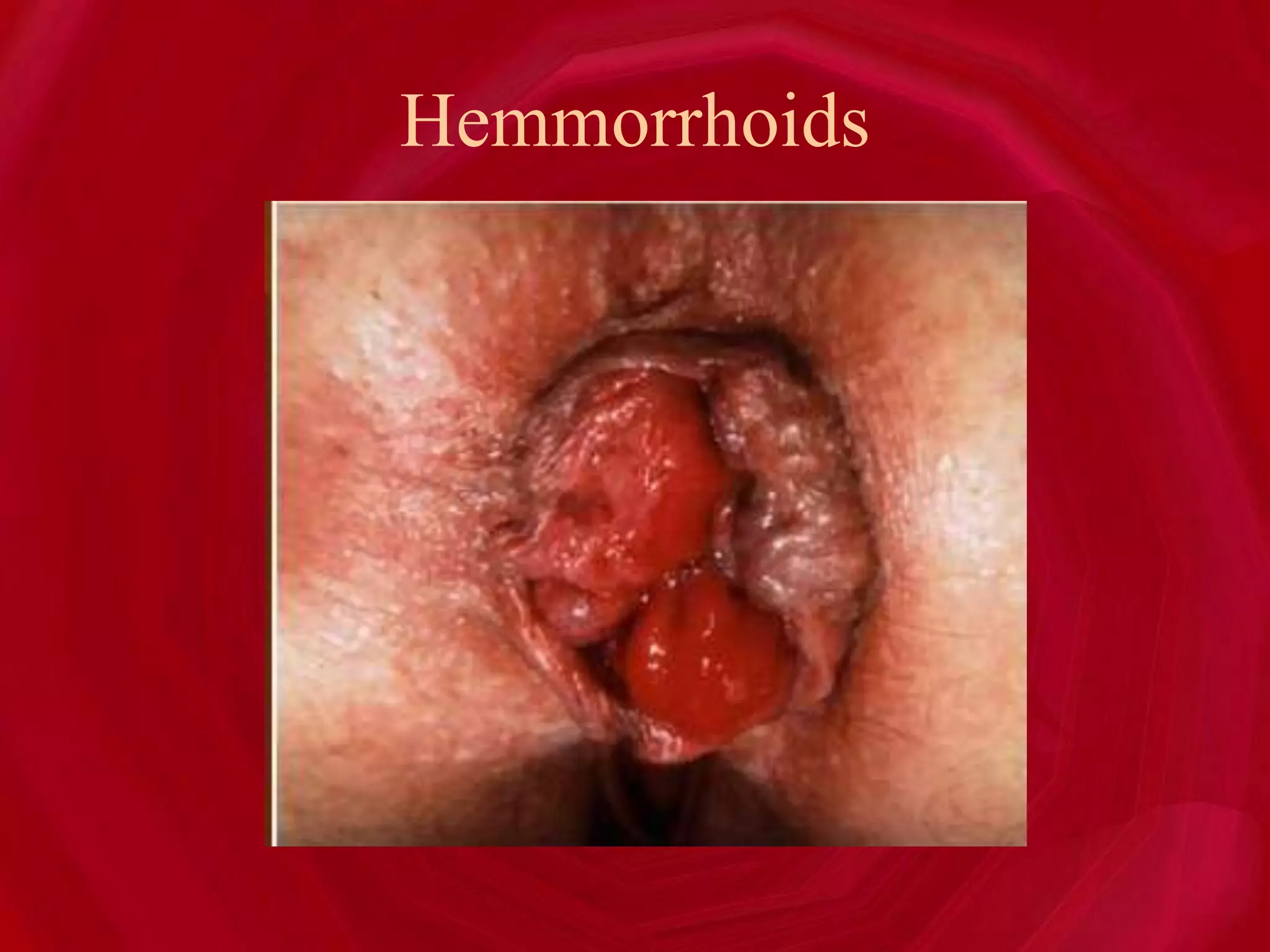
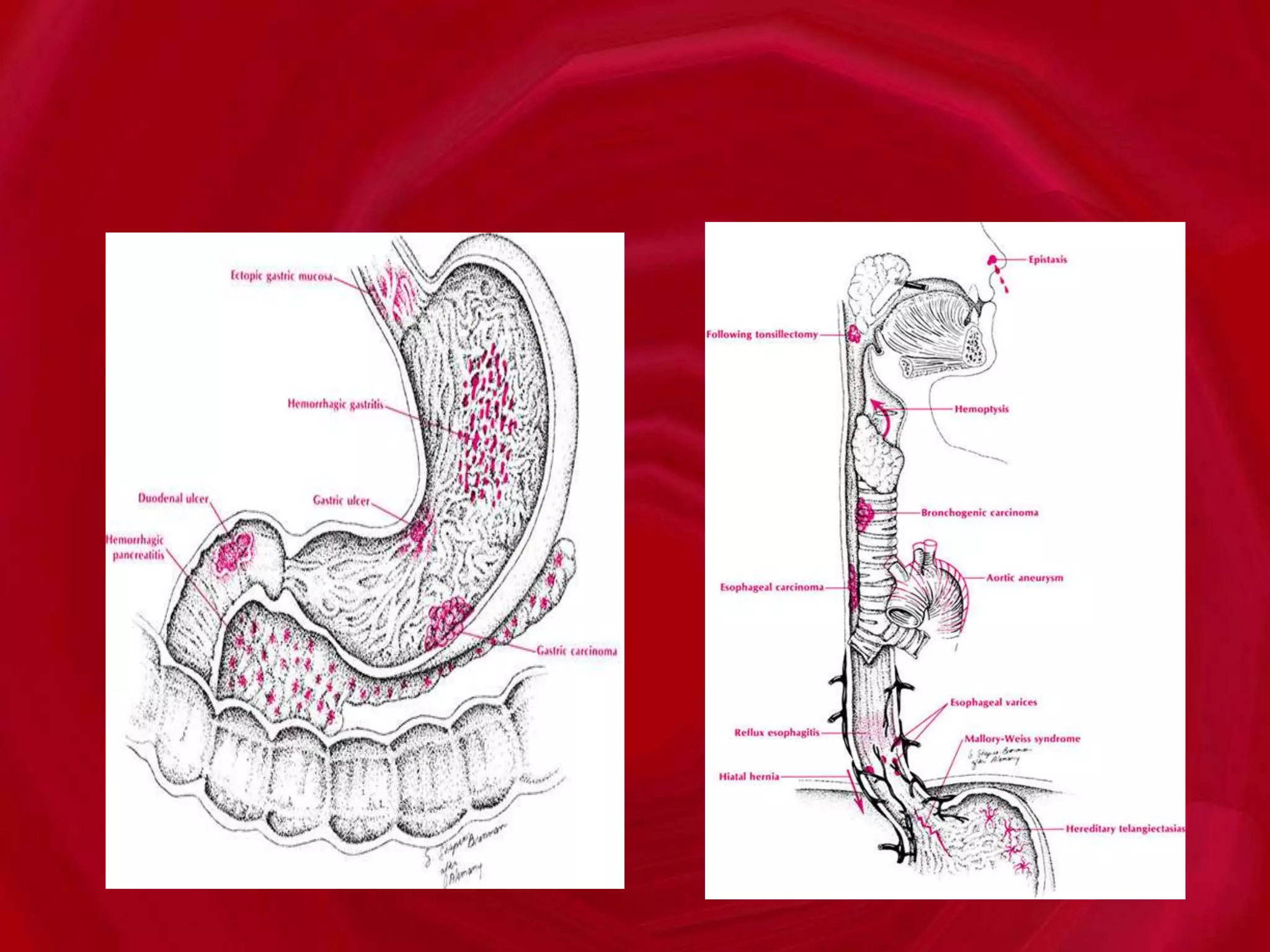
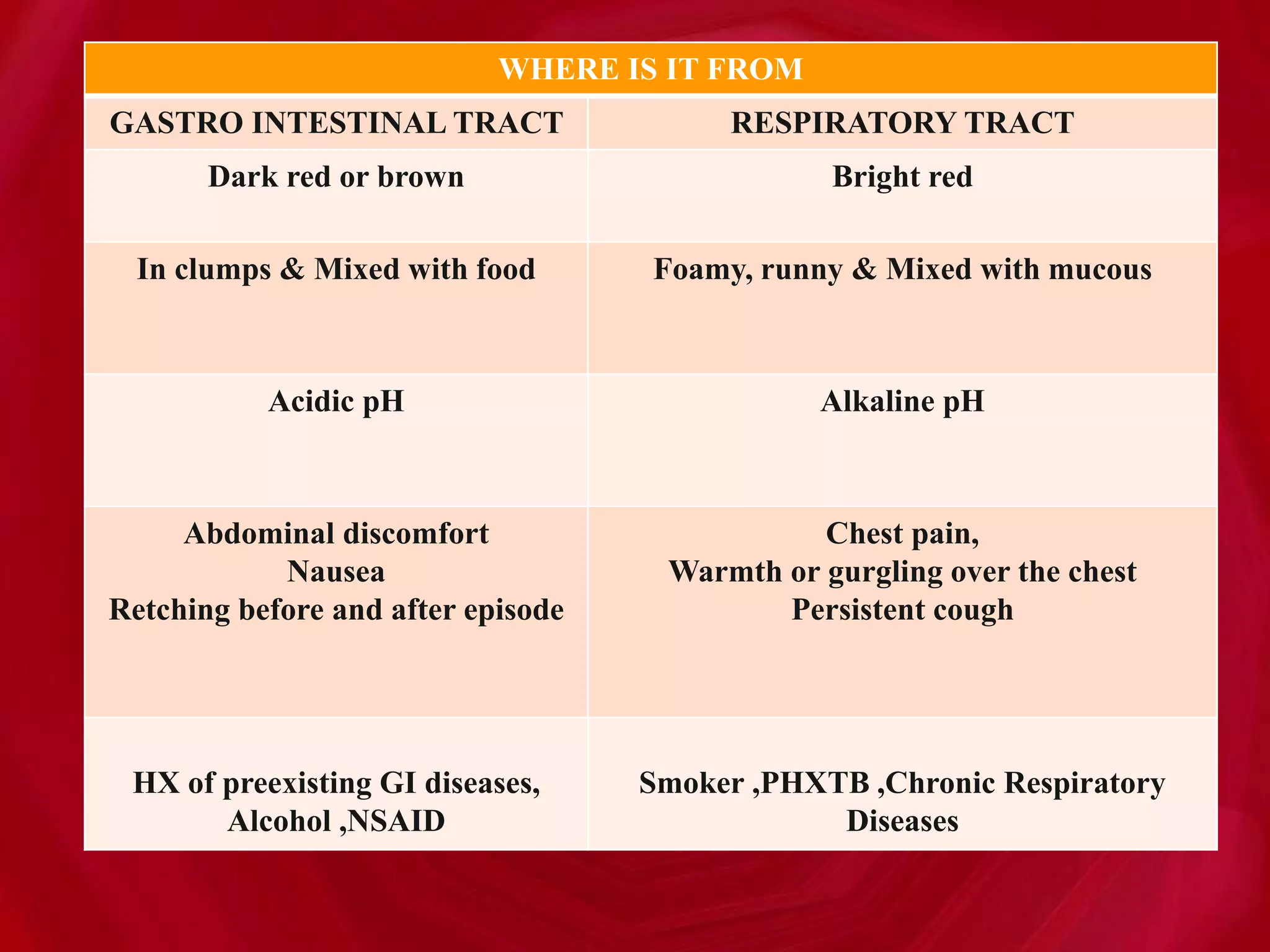
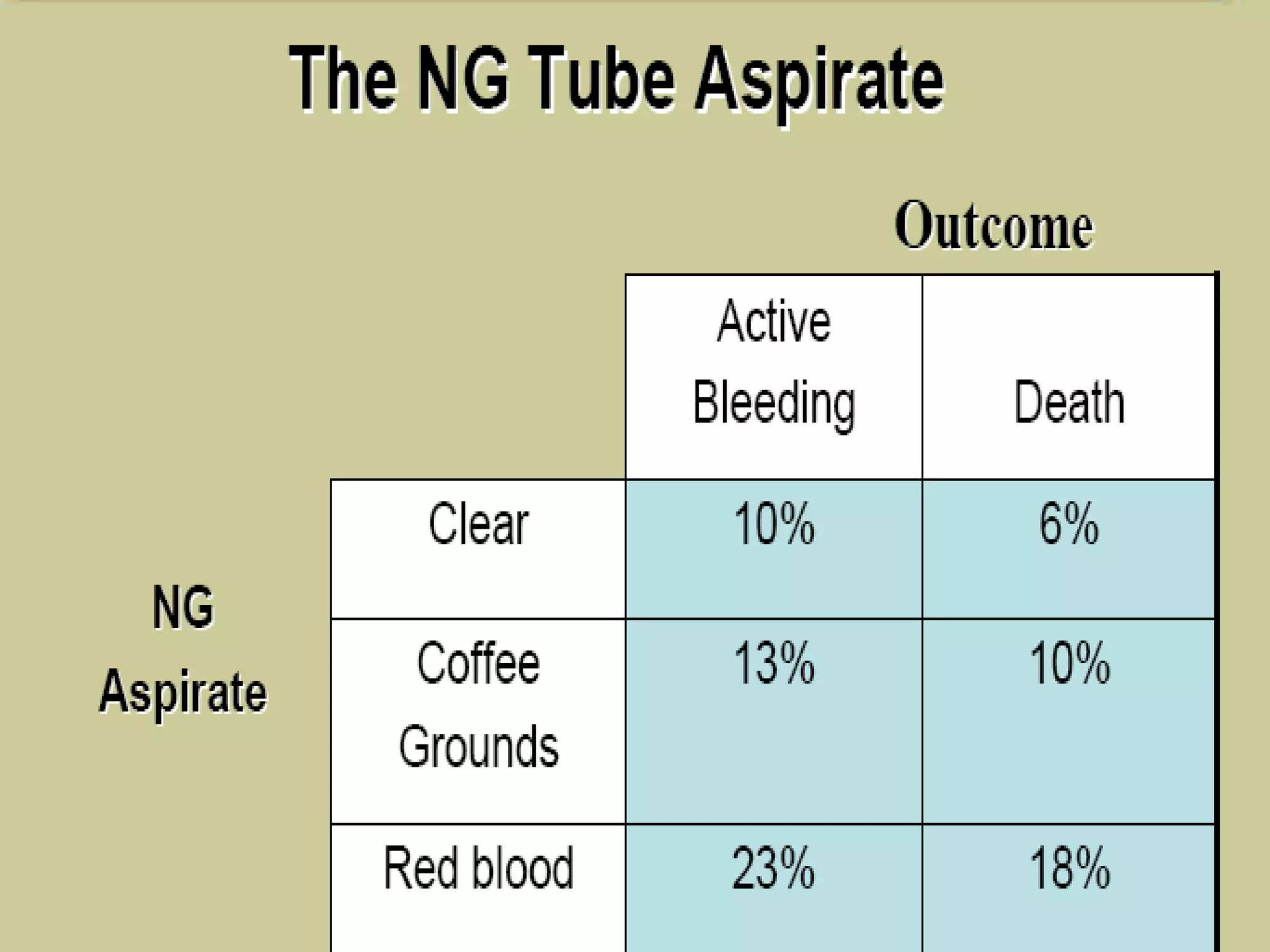
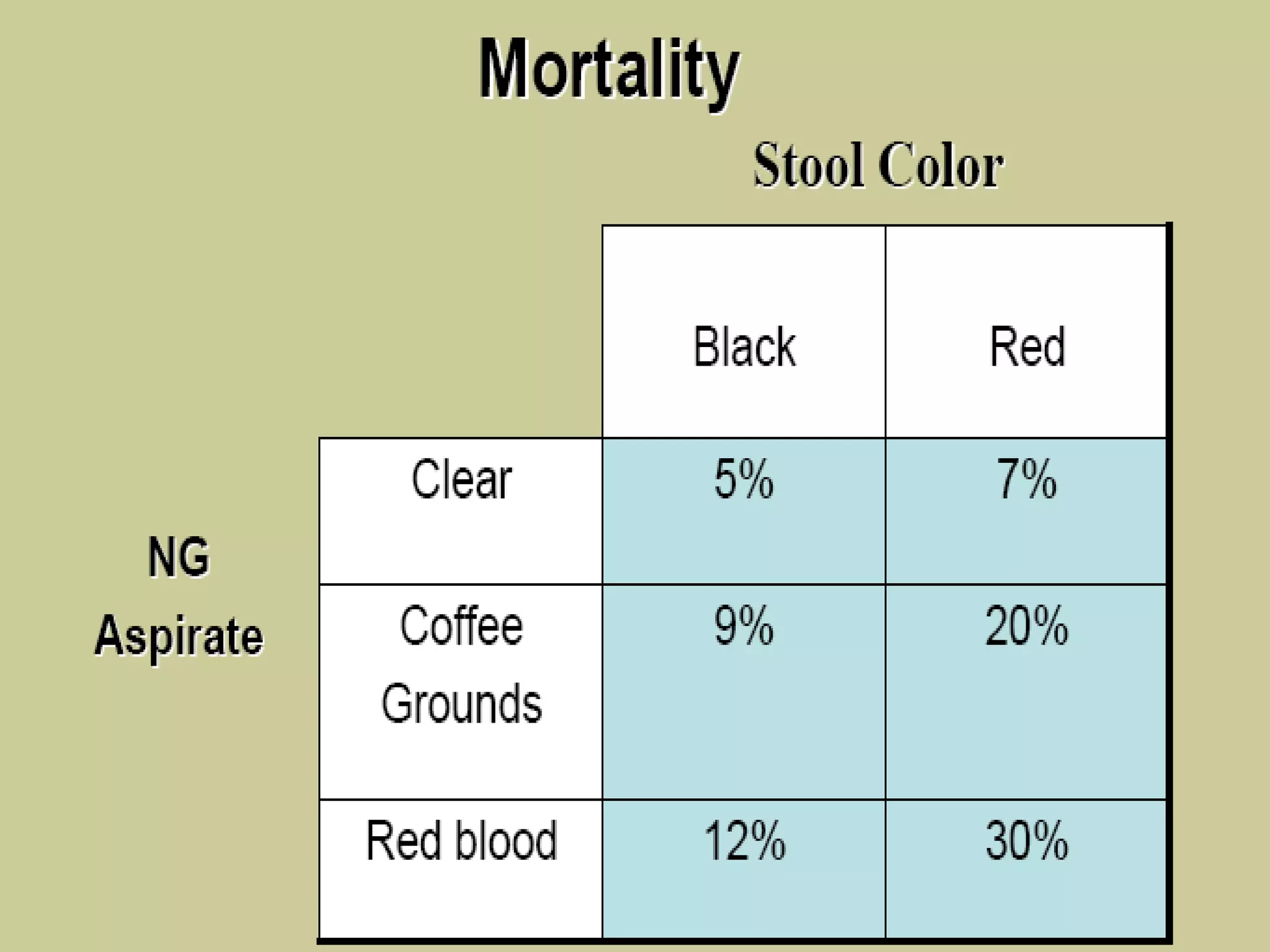
- Clinical presentations of GI bleeding include hematemesis, melena, hematochezia, occult bleeding, and symptoms of blood loss/anemia.
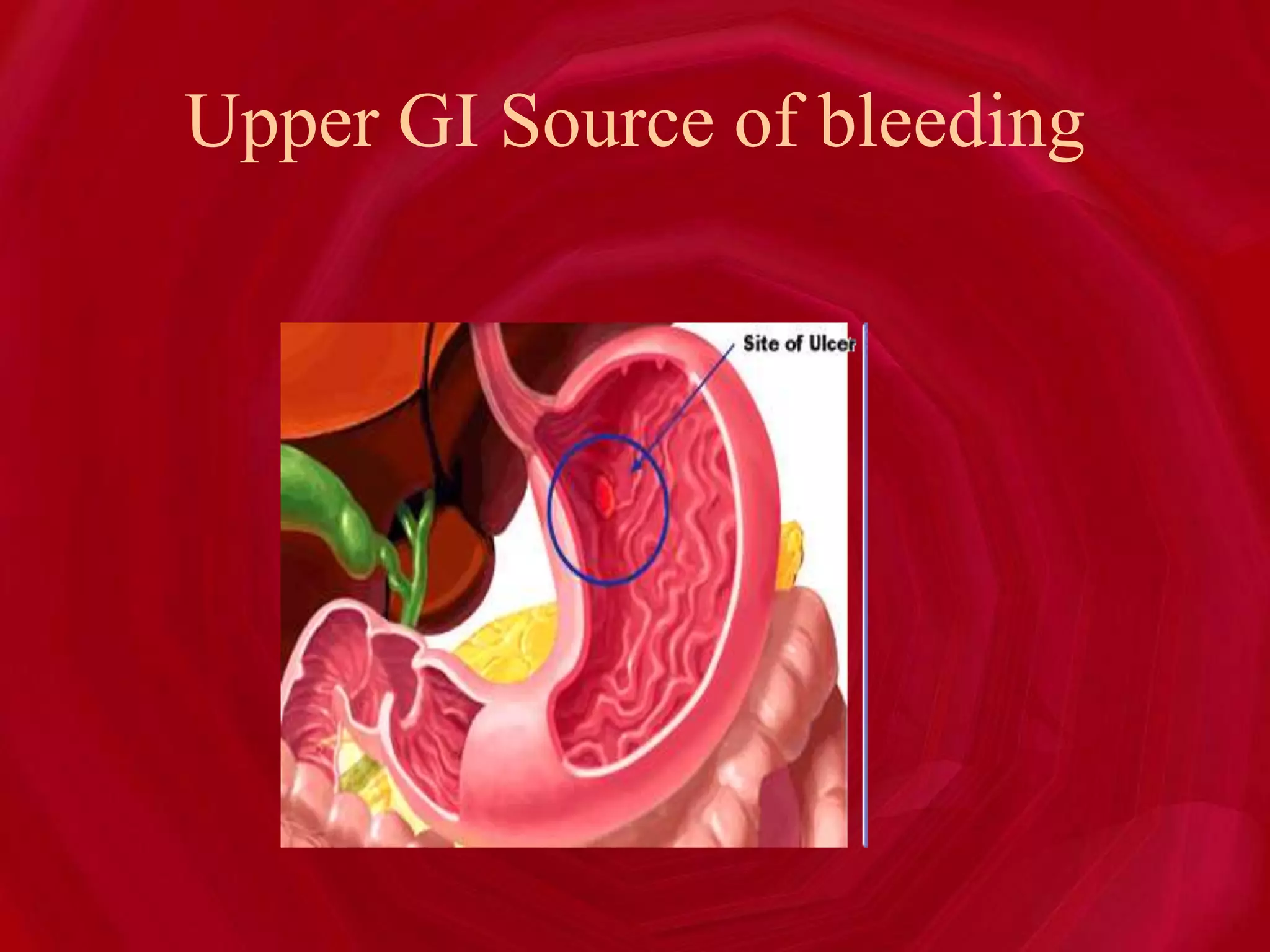
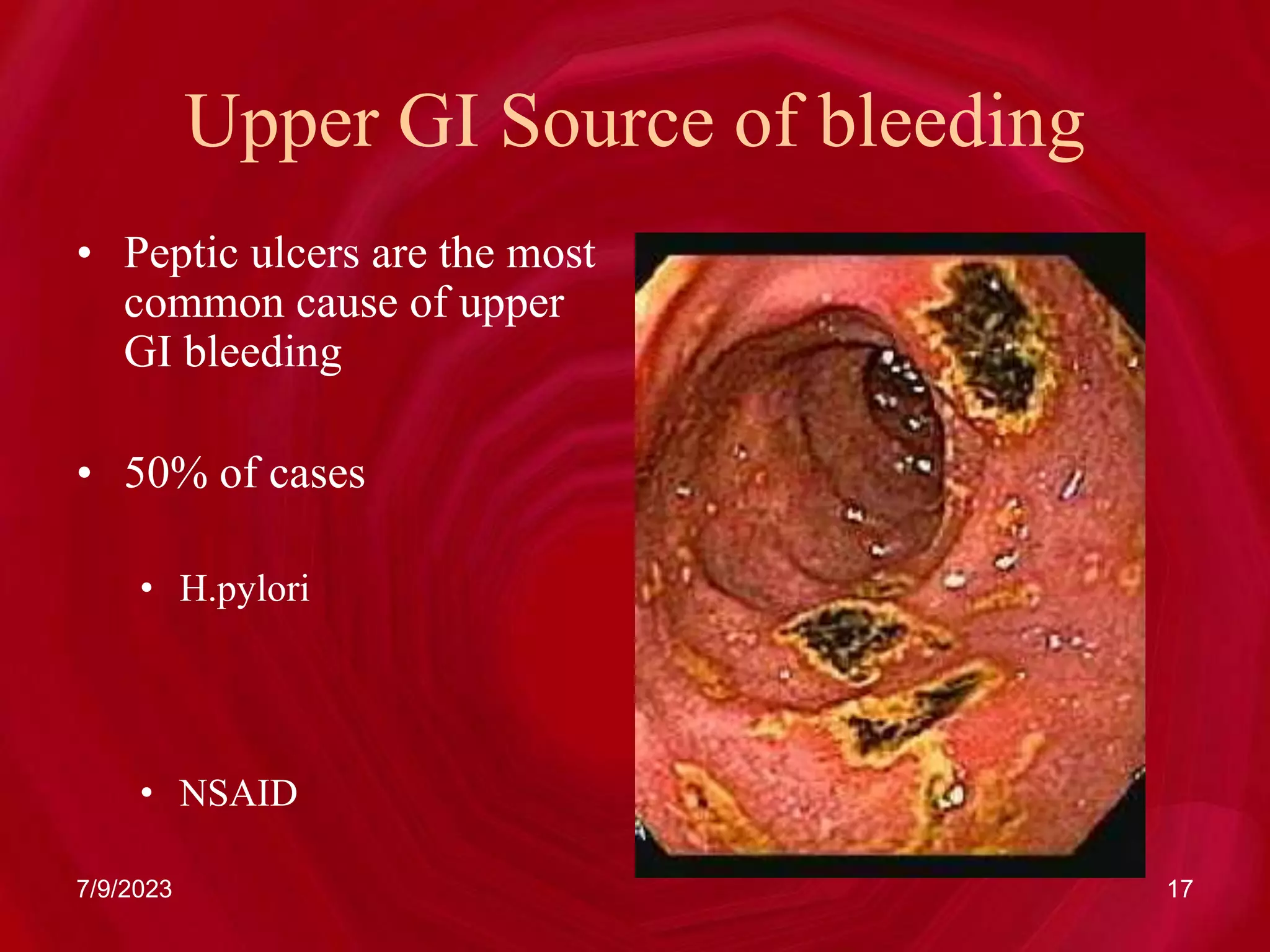
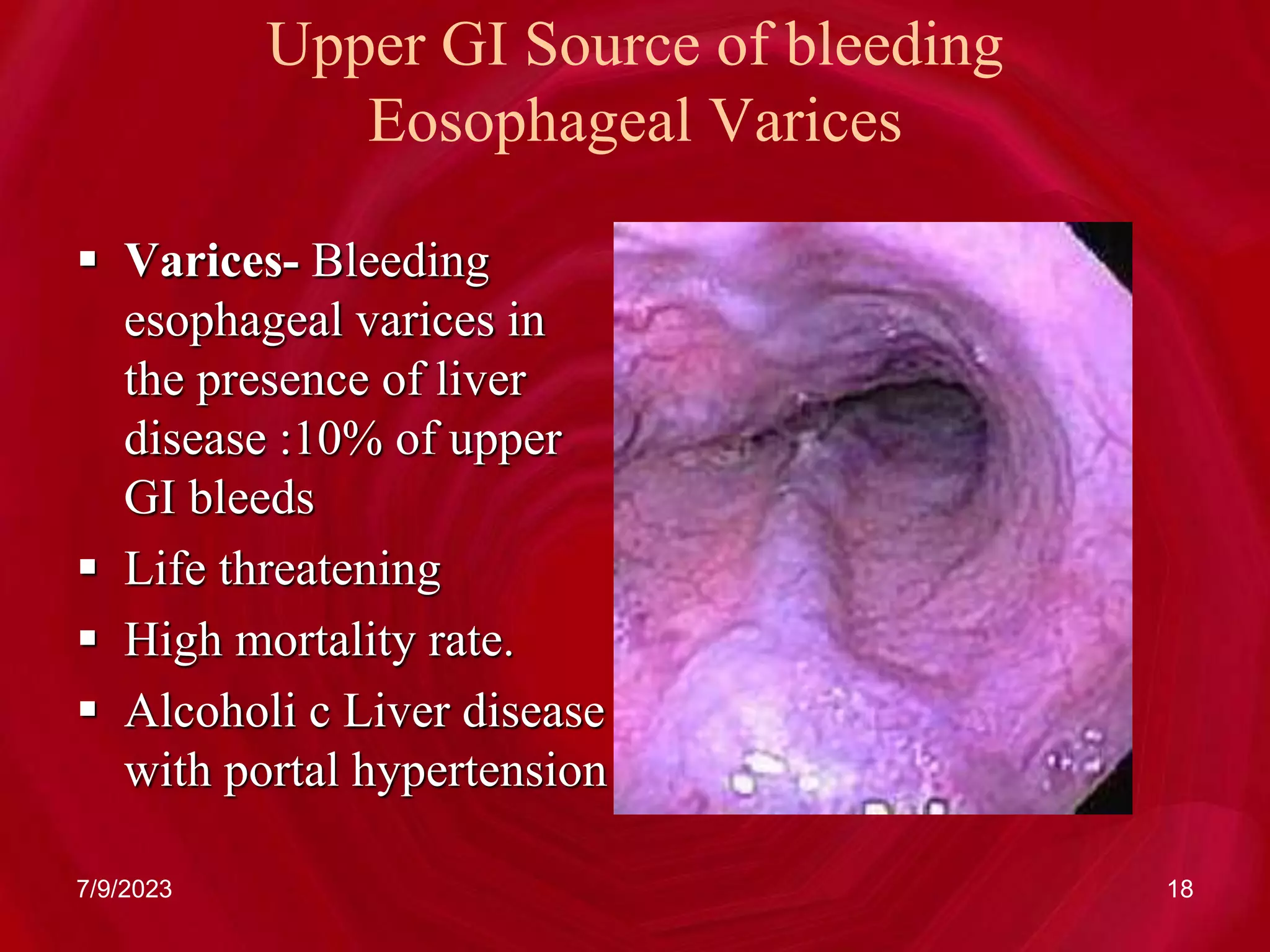
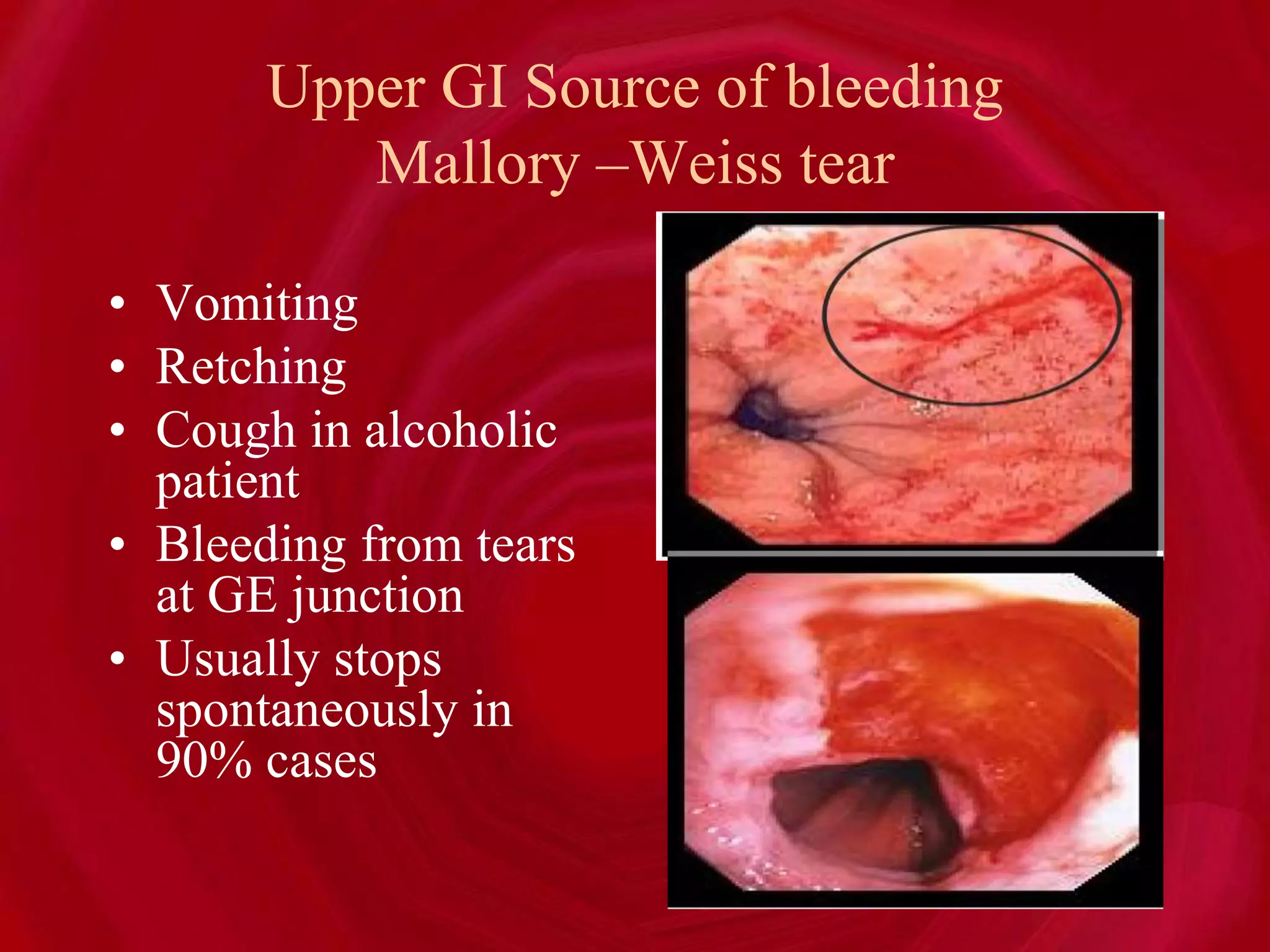
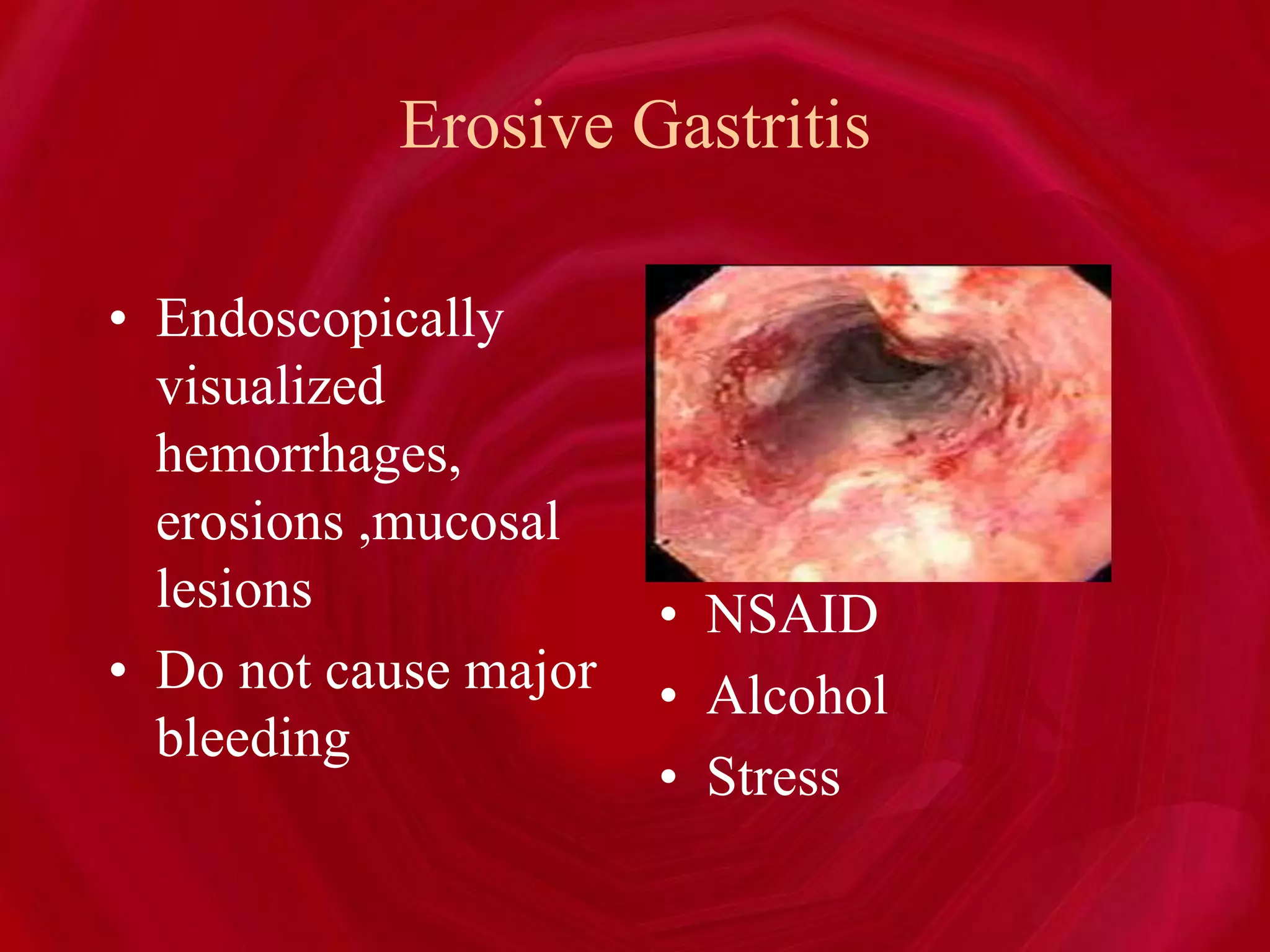
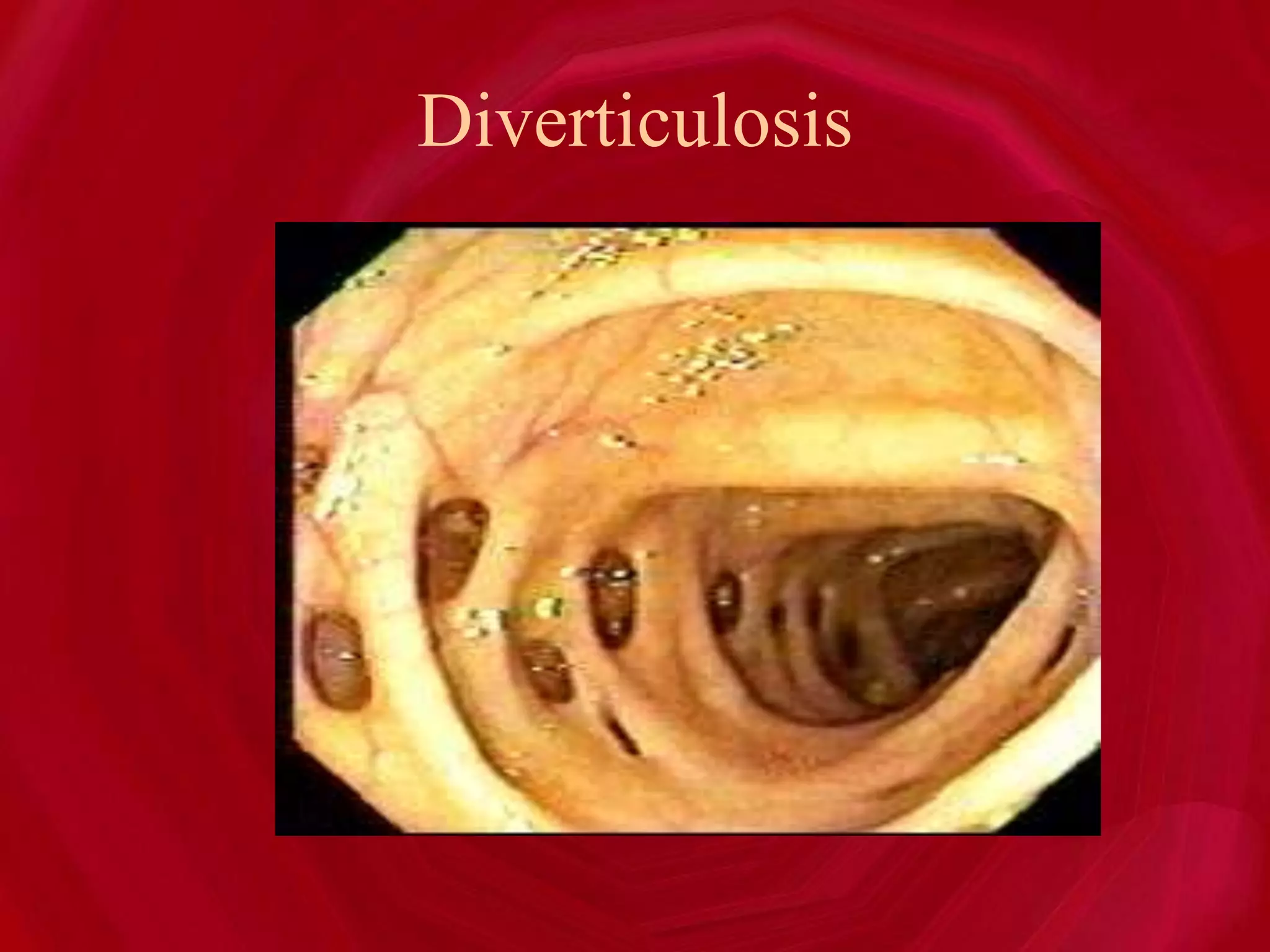
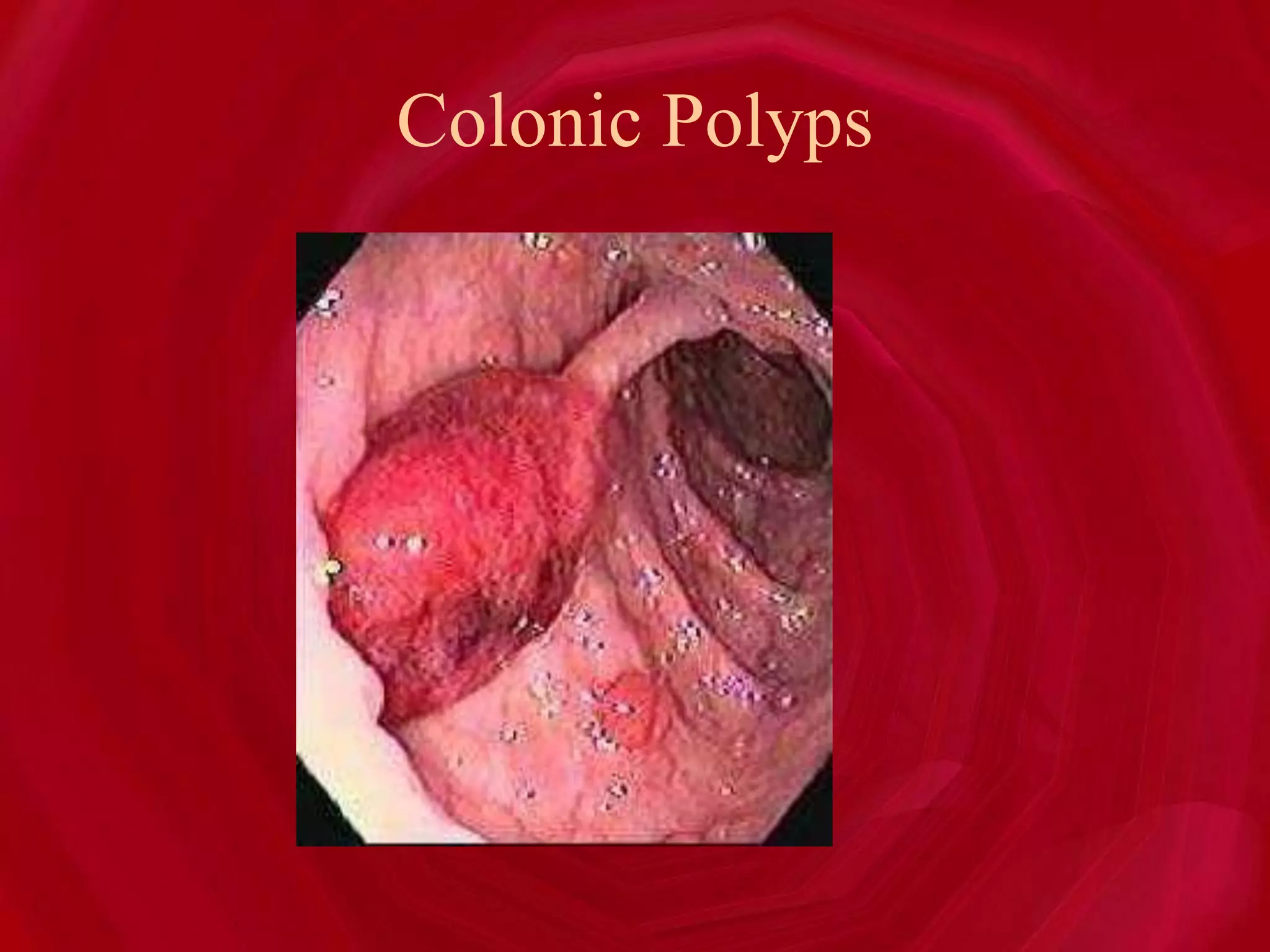
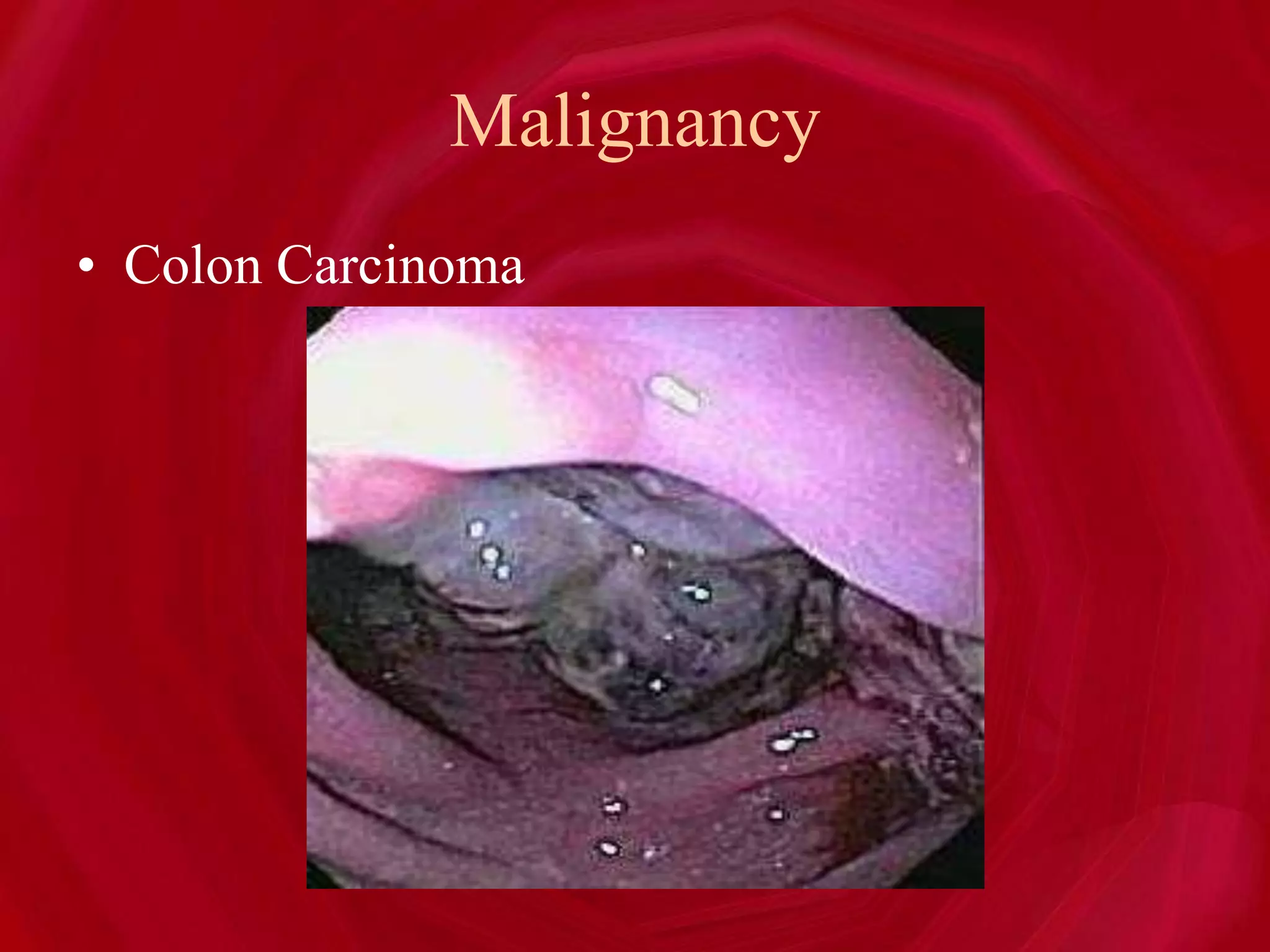
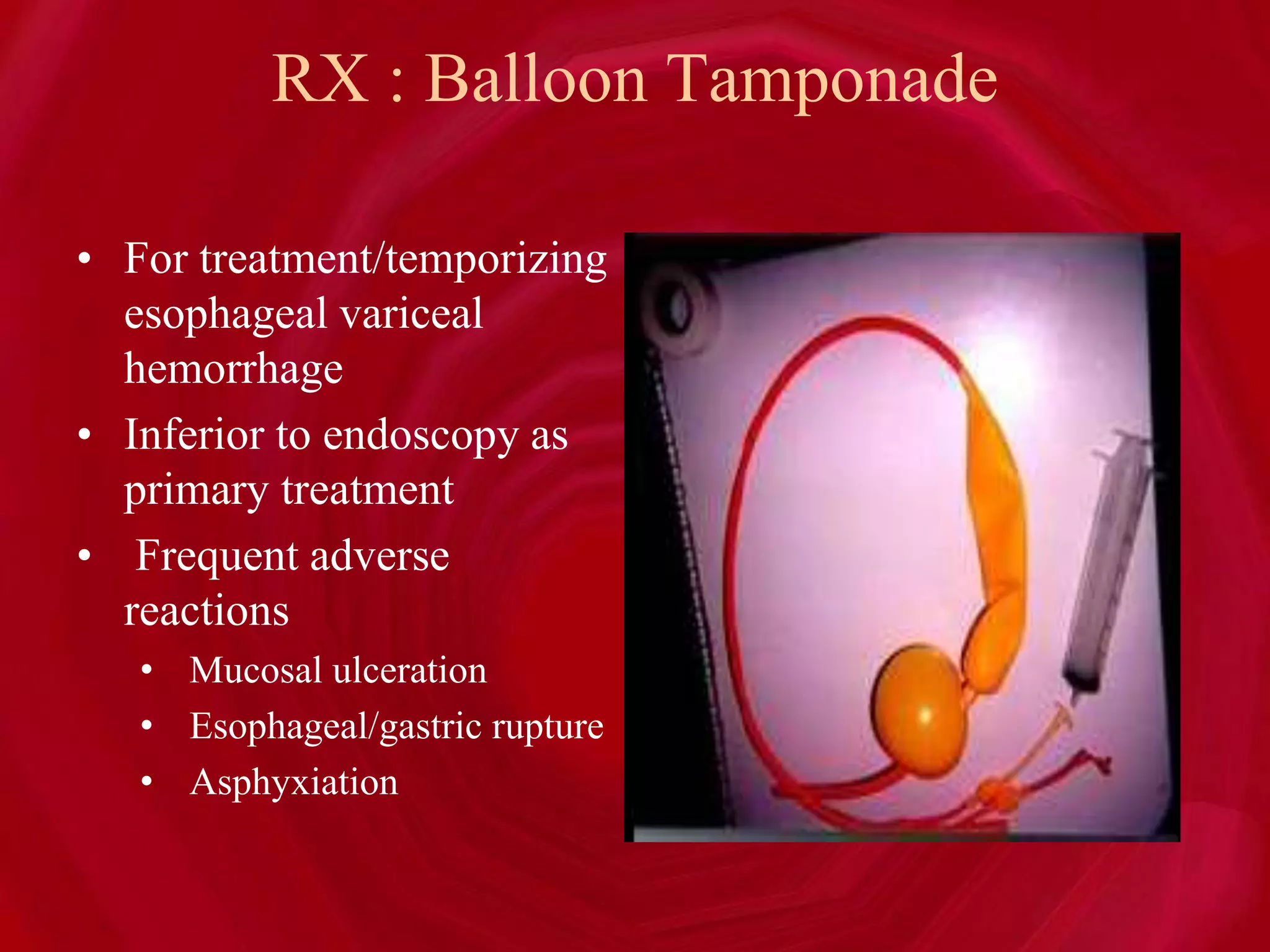
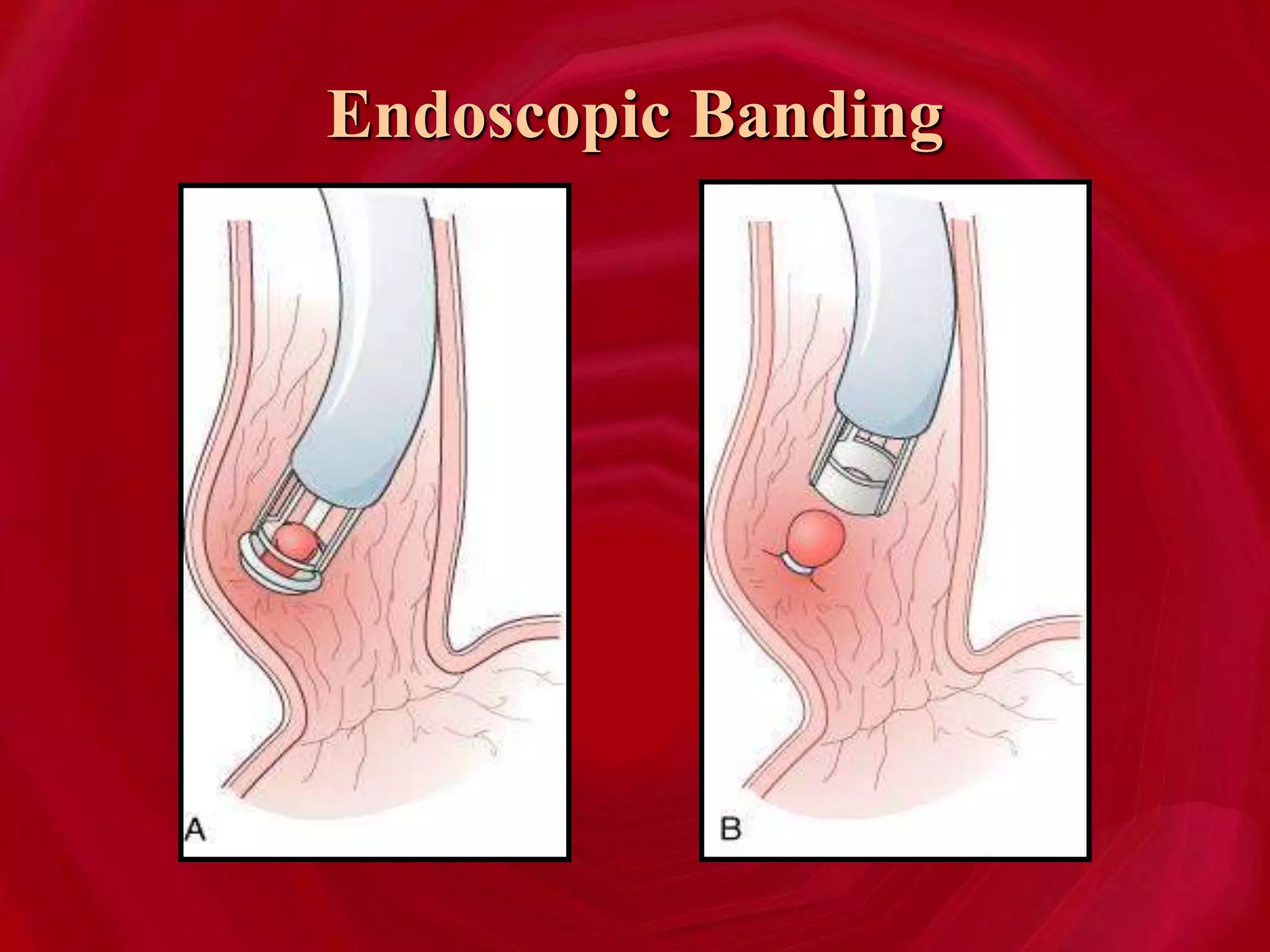
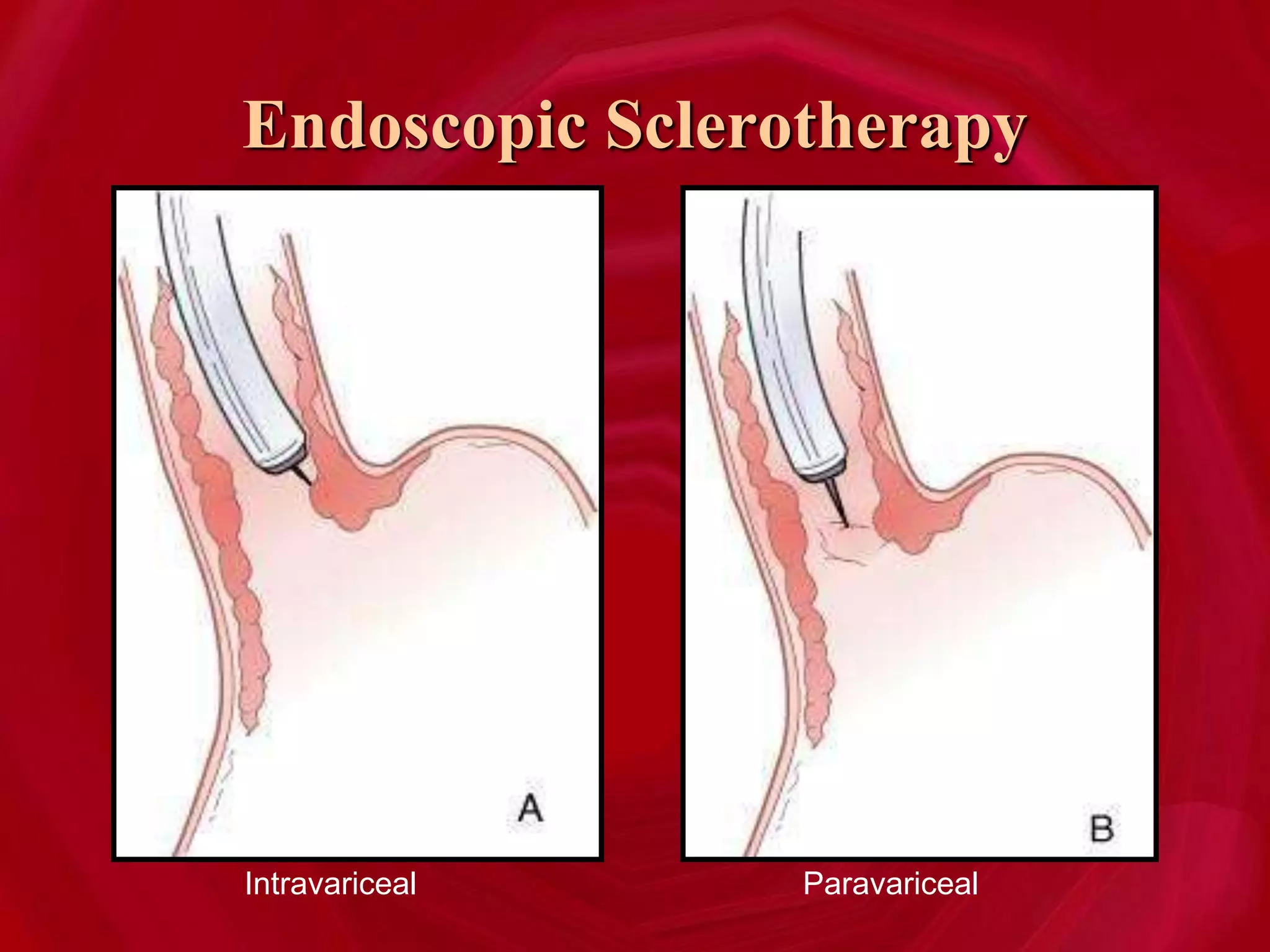
- Common causes of upper GI bleeding are peptic ulcers and esophageal varices, while diverticulosis and colon polyps are common causes of lower GI bleeding.
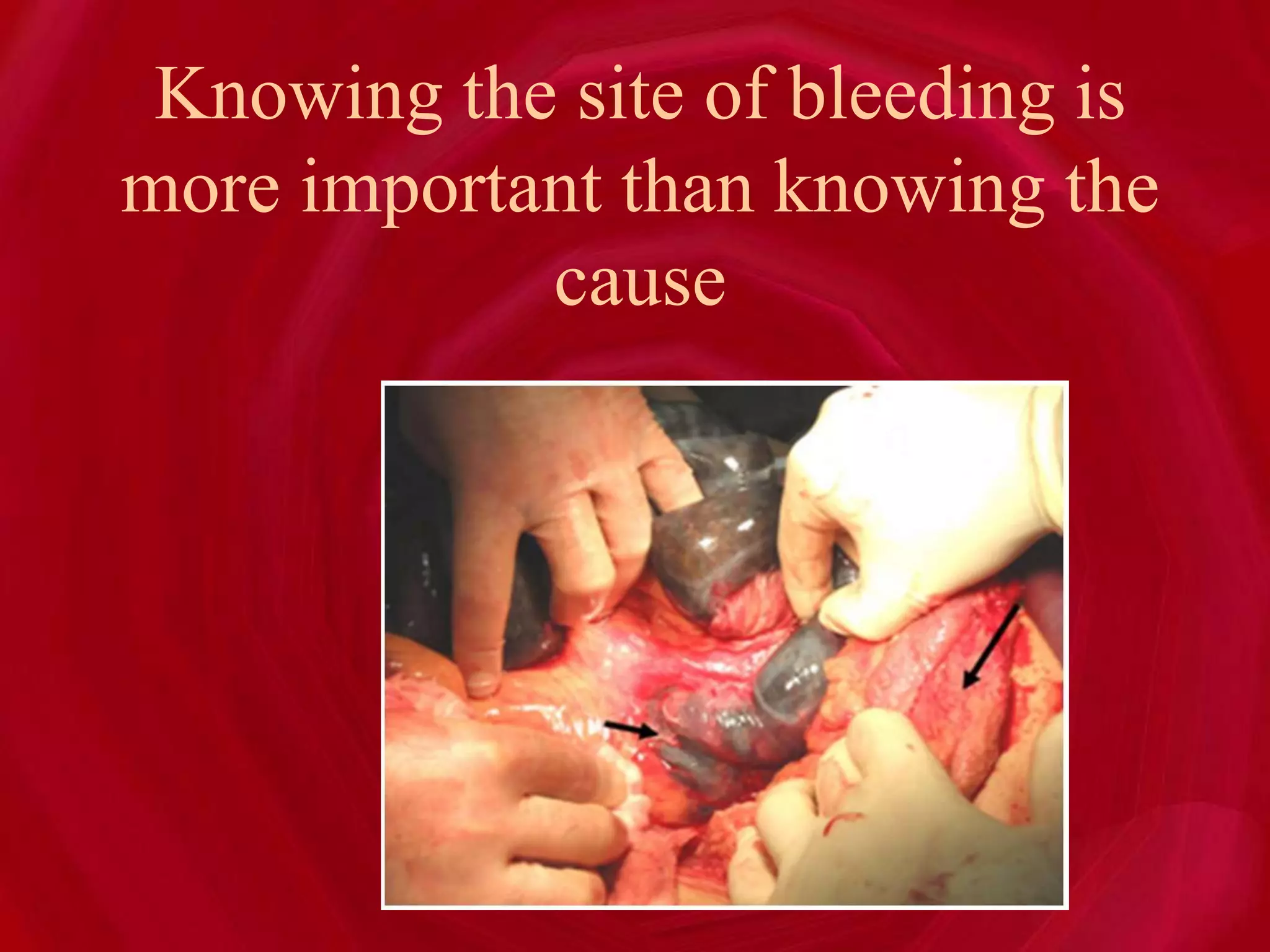
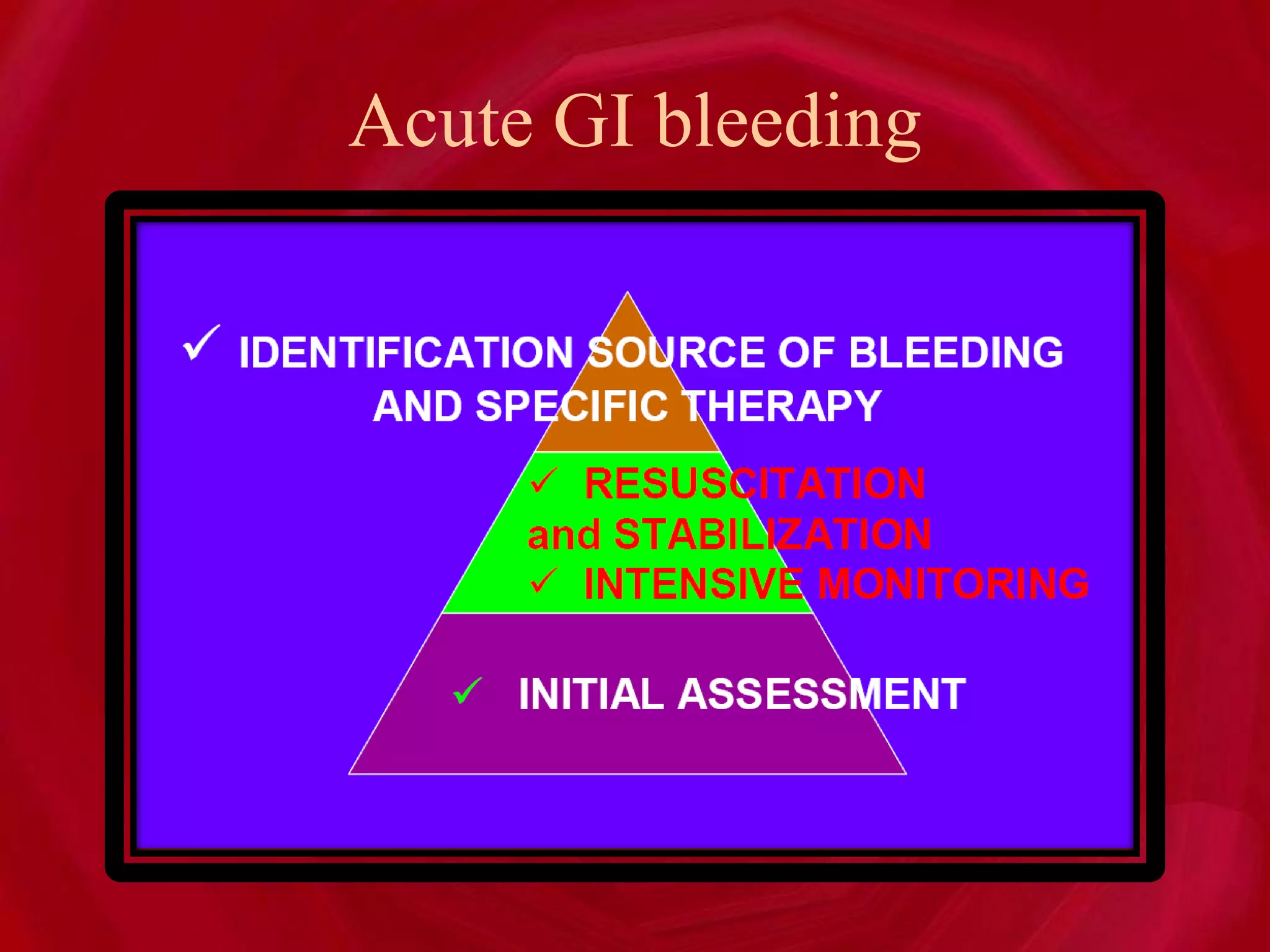
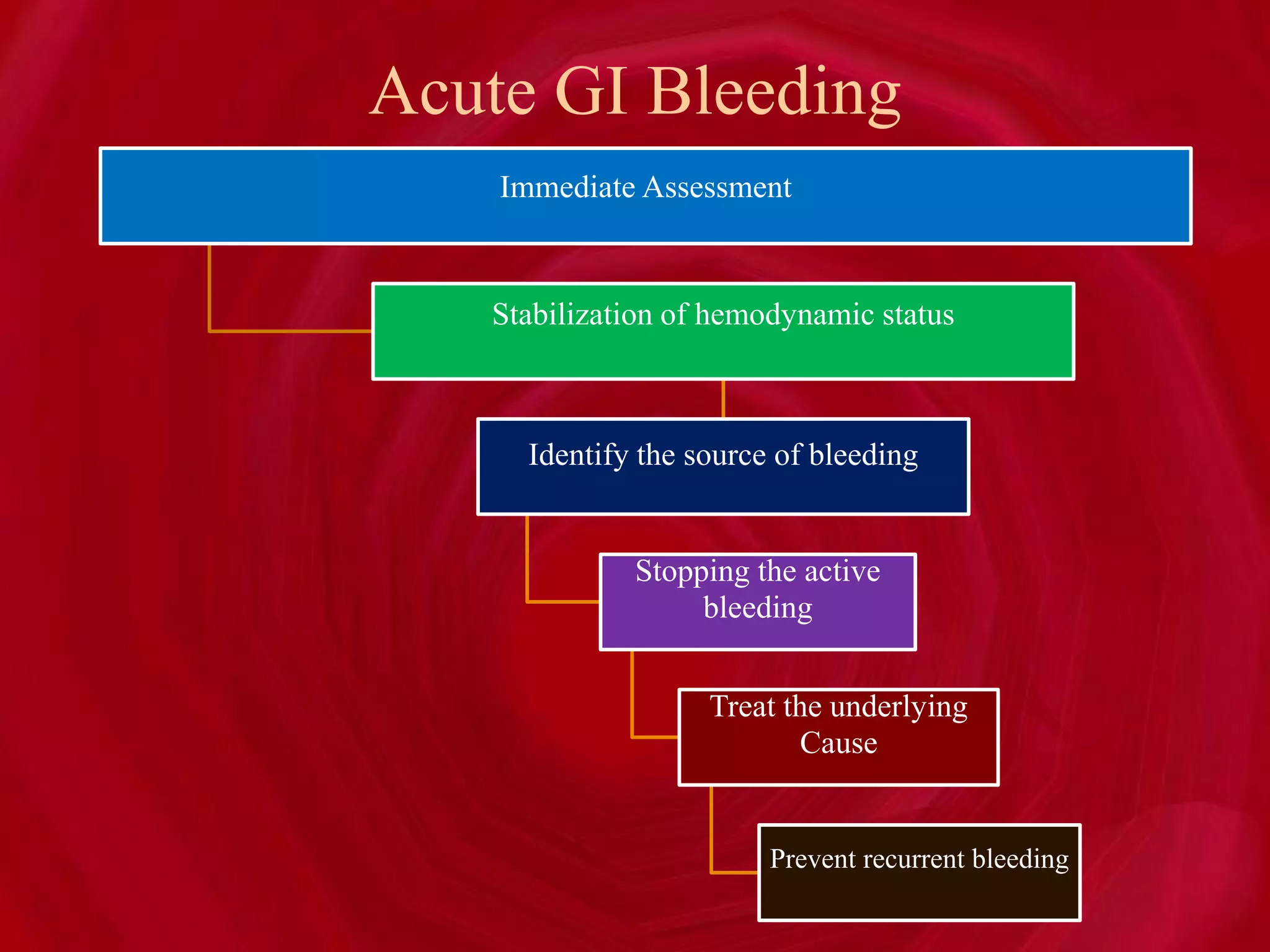
- The approach to a patient with GI bleeding involves stabilizing their hemodynamic status, identifying the source of bleeding, stopping active bleeding, treating the underlying cause, and preventing recurrent







































![GASTROINTESTINAL BLEED ARUP SIR [Autosaved] copy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gastrointestinalbleed-arupsirautosavedcopy-250402060103-4e590a88-thumbnail.jpg?width=640&height=640&fit=bounds)




















![HIGH ALTITUDE PULMONORY EDEMA (HAPE)[2305843009213699724].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/highaltitudepulmonoryedemahape2305843009213699724-230505035742-4455e82f-thumbnail.jpg?width=640&height=640&fit=bounds)























