GI BLEEDING
Gastrointestinal bleeding(GIB) is a
term that describes the loss of blood
from along the alimentary canal.
GIB is classified by its anatomic
location relative to the ligament of
Treitz.
Upper GIB (UGIB) is defined as being
proximal to the ligament of Treitz.
3.
GI BLEEDING
Upper intestinalhemorrhage is the most common presentation of
GIB and is commonly from peptic ulcer disease (PUD) or oesophageal
varices. Pancreatic, liver, and other biliary origins of blood loss also are
encompassed by this term.
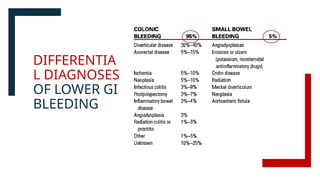
Lower GIB (LGIB) accounts for 30% to 40% of all bleeds and is defined
as distal to the ligament of Treitz. This most often originates from the
colon from diverticular disease or angiodysplasias.
The term massive GIB refers to intestinal blood loss leading to
hemodynamic instability or transfusion requirement, whereas occult
GIB refers to anemia that persists or recurs after negative endoscopic
evaluation and imaging workup.
LOWER GI BLEEDING
Bleedingfrom the GI tract distal to the ligament of Treitz,
mainly from the small intestine, colon, rectum, or anus.
Normal faecal blood loss is 1.2 ml/day. A loss more than 10
ml/day is significant.
Incidence:
Accounts for 30% to 40% of all GI bleeds.
More common in elderly patients and those with comorbidities.
Severity: Can range from self-limiting to life-threatening
hemorrhage requiring surgical intervention
CLASSIFICATION
B. Based onsite:
1. Small bowel bleed: Polyps, Meckel’s diverticulum,
mesenteric ischaemia, intussusception; small bowel
tumor.
2.Large bowel bleed: Angiodysplasia, carcinoma,
colitis, diverticulitis, carcinoma.
3.Anorectal diseases: Piles, fissure-in-ano,
carcinomas.
10.
CLASSIFICATION
C. Based onintensity :
1.Massive bleeding: Bleeding> 1.5l/day. Associated
hemodynamic instability(HOTN, tachycardia). Need blood
transfusion of greater than 2U.
2.Moderate bleeding: No significant hemodynamic
instability. May require transfusion but usually responds to
conservative management.
3.Occult bleeding: >10 ml/day but not revealed. No
hemodynamic instability.
11.
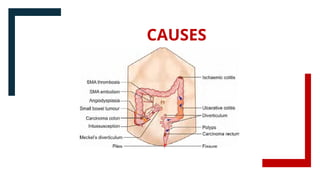
CAUSES
Angiodysplasia.
Diverticulardisease
(commonest cause in Western
countries.)
Tumours of colon or small
bowel.
Anorectal
diseases(haemorrhoids, fissure-
in-ano)
Ulcerative colitis, Crohn’s
disease.
Colorectal polyps; rectal
carcinomas.
Intussusception.
Tumours, either benign or
malignant of colon or small
bowel.
Meckel’s diverticulum.
Ischaemic colitis.
Stercoral ulcer.
Infectious colitis.
Mesenteric artery occlusion.
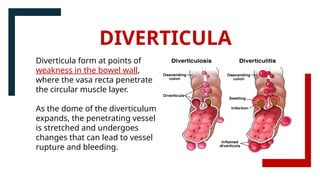
Diverticula form atpoints of
weakness in the bowel wall,
where the vasa recta penetrate
the circular muscle layer.
As the dome of the diverticulum
expands, the penetrating vessel
is stretched and undergoes
changes that can lead to vessel
rupture and bleeding.
DIVERTICULA
14.
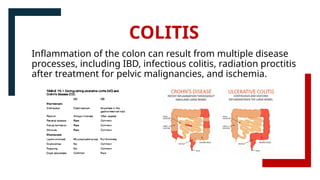
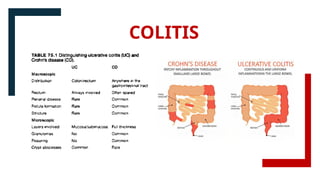
COLITIS
Inflammation of thecolon can result from multiple disease
processes, including IBD, infectious colitis, radiation proctitis
after treatment for pelvic malignancies, and ischemia.
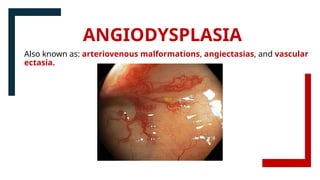
ANGIODYSPLASIA
Also known as:arteriovenous malformations,
angiectasias, and vascular ectasia.
Vascular abnormality of GIT characterised by
dilated, thin walled blood vessels in mucosa and
submucosa.
Commonly occurs in the right colon (cecum and
ascending colon)
The presentation is similar to diverticular bleeding
in that it is painless, usually self-limiting, and
intermittent. Unlike diverticular bleeding, this tends
to be venous bleeding.
Associated with aging, chronic kidney disease, von
Willebrand disease, and aortic stenosis (Heyde
syndrome).
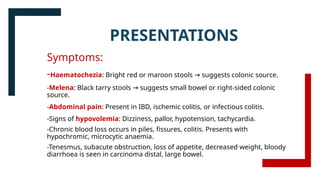
PRESENTATIONS
Symptoms:
-Haematochezia: Bright redor maroon stools suggests colonic source.
→
-Melena: Black tarry stools suggests small bowel or right-sided colonic
→
source.
-Abdominal pain: Present in IBD, ischemic colitis, or infectious colitis.
-Signs of hypovolemia: Dizziness, pallor, hypotension, tachycardia.
-Chronic blood loss occurs in piles, fissures, colitis. Presents with
hypochromic, microcytic anaemia.
-Tenesmus, subacute obstruction, loss of appetite, decreased weight, bloody
diarrhoea is seen in carcinoma distal, large bowel.
19.
Signs on Examination
-Abdominalexam: Tenderness (IBD, ischemia), distension
(obstruction), mass palpable in left or right iliac fossa or mass
of intussusception
-Per-rectal examination: Hemorrhoids, masses, fissures, or
blood in the rectum.
Blood with mucus—colitis, carcinoma
Fresh blood as splashes in the pan—piles
Maroon coloured stool—Meckel's diverticulum
Red currant jelly in stool—intussusception
Bright red blood in stool—polyps
PRESENTATIONS
20.
MANAGEMENT
INITIAL STABILIZATION (Resuscitationand supportive care)
Rapid triage of hemorrhaging patients while localizing the areas of blood
loss is essential for resuscitation and prompt intervention.
1.The ABCDEs
2.IV Access and Monitoring
Establish two large-bore IV lines(14- or 16- gauge)
Consider central access for massive hemorrhage
Urinary catheter placed to monitor resuscitation adequacy
3.Recognizing severe hemorrhage
Hypotension(SBP<90 mmHg) suggests>30% blood loss.
Tachypnea, tachycardia, hypotension, agitation, and mental status changes are all
indicators of a severe degree of hemorrhage.
21.
4.Additional management priorities:
Typeand crossmatch,CBC, metabolic panel, coagulation profile, LFT.
Serum lactate can be utilized as an endpoint of resuscitation when
elevated.
5.Fluid Resuscitation and Transfusion Strategy:
Massive transfusion protocol for severe hemorrhage
Blood Transfusion: Hb <7 g/dL (stable) or <9 g/dL (unstable/cardiac
disease).
Monitor coagulation(PT, PTT, fibrinogen, platelets)
Use of rapid infuser to prevent hypothermia.
MANAGEMENT
22.
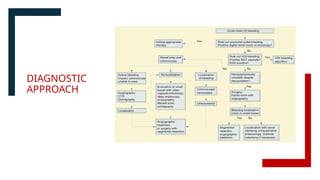
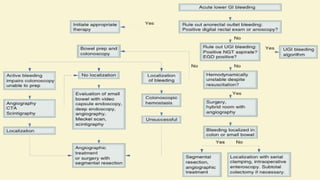
DIAGNOSTIC APPROACH
Step 1:Initial Clinical Assessment
1.1 History
Age & Risk Factors:
Elderly: Diverticulosis, ischemic colitis, angiodysplasia, colorectal
cancer.
Young Adults: IBD, haemorrhoids, infectious colitis.
Nature of Bleeding:
Bright red blood per rectum (haematochezia): Distal colonic or rectal source.
Maroon- coloured stools: Right colon or small bowel source.
Melena (black, tarry stools): Upper GI or proximal small bowel source.
23.
Associated Symptoms:
Abdominal pain:IBD, ischemic colitis, diverticulitis.
Diarrhea: Infectious colitis, IBD.
Tenesmus: Rectal malignancy, ulcerative colitis.
Weight loss, altered bowel habits: Suggests malignancy.
Medication History:
NSAIDs, aspirin: Risk of diverticular bleeding, peptic ulcer
disease.
Anticoagulants (Warfarin, DOACs): Increased risk of severe
bleeding.
Past Medical History:
History of radiation therapy: Radiation proctitis.
Atherosclerosis, cardiovascular disease: Ischemic colitis.
Step 2: LaboratoryInvestigations
•CBC:
-Anemia (Hb <7 g/dL transfusion needed).
→
-Leukocytosis (infection, IBD, ischemia).
•Coagulation Profile: INR, PT, APTT (for anticoagulant-induced bleeding).
•Electrolytes & Renal Function: Hypovolemia-induced acute kidney injury.
•Liver Function Tests: Rule out coagulopathy due to liver disease.
•Stool Studies: Occult blood test, fecal calprotectin (IBD), C. Difficile toxin
assay.
•Type & Crossmatch: Prepare for transfusion in case of significant bleeding.
28.
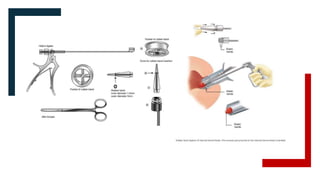
Step 3: Imaging& Endoscopy
3.1 Colonoscopy (Gold Standard)
Best for stable patients after initial resuscitation.
Can diagnose and treat diverticular disease, angiodysplasia,
IBD, colorectal cancer.
Findings: Diverticulosis: Outpouchings, active bleeding site.
IBD: Mucosal inflammation, ulcerations.
3.2 CT Angiography (CTA) :When endoscopy is unable to
localize a LGIB, angiography is an important diagnostic as well
as therapeutic tool.
Preferred in active bleeding (>0.3–0.5 mL/min).
Findings: Contrast extravasation = active bleeding site. Vascular
malformations (angiodysplasia).
29.
Step 3: Imaging& Endoscopy
3.3 Radionuclide Scintigraphy (Tagged RBC
Scan)
Detects slower, intermittent bleeding (>0.1
mL/min).Useful when colonoscopy is non-
diagnostic.
3.4 Capsule Endoscopy
For obscure GI bleeding (if upper & lower
endoscopy are normal).
Detects small bowel lesions
(angiodysplasia, Crohn’s disease).
30.
Step 4. DefinitiveManagement
4.1: Endoscopic Therapy (First-line for Most Cases)
Hemostatic Clipping: Preferred for diverticular bleeding, angiodysplasia.
Thermal Coagulation: Used for bleeding ulcers, angiodysplasia.
Epinephrine Injection: Provides temporary vasoconstriction
Band Ligation: For bleeding internal hemorrhoids.
4.2: Angiographic Embolization
Indications: Persistent bleeding despite endoscopy. Patients unfit for
surgery.
Procedure:
Super-selective embolization of bleeding artery (SMA, IMA branches).
Agents: Gelatin sponge, coils, or polyvinyl alcohol (PVA) particles.
31.
Step 4. Definitive
Management
4.1:Endoscopic Therapy (First-line for Most
Cases)
Hemostatic Clipping: Preferred for
diverticular bleeding, angiodysplasia.
Thermal Coagulation: Used for
bleeding ulcers, angiodysplasia.
Epinephrine Injection: Provides
temporary vasoconstriction
Band Ligation: For bleeding internal
hemorrhoids.
33.
Step 4. Definitive
Management
4.3:Medical Therapy
•Proton Pump Inhibitors (PPIs):
Used in peptic ulcer disease, gastric
protection.
•Octreotide: Used in variceal
bleeding (portal hypertension).
•Antibiotics: Metronidazole +
Ciprofloxacin for infectious colitis.
Vancomycin PO for C. Difficile colitis.
34.
Step 4. DefinitiveManagement
4.4: Surgical Intervention (Last Resort)
Indications: Persistent hemodynamic instability despite resuscitation attempts
or administering more than 4 units of blood in 24 hours or more than10 units
of blood during the hospital stay are considered indications for surgery
Surgical Options:
Segmental Colectomy: If the source is localized (e.g., single diverticulum).
Subtotal Colectomy: If diffuse bleeding or unable to identify the source.
Proctocolectomy: For severe ulcerative colitis.
Note:Preoperative identification of the culprit lesion is particularly important in LGIB
because, without localization, the empiric surgery for unlocalized LGIB is a total
abdominal colectomy and end ileostomy.
#2 the ligament of Treitz. : right crus of diaphragm to duodenjejunal flexure
#3 the ligament of Treitz. : right crus of diaphragm to duodenjejunal flexure
#4 the ligament of Treitz. : right crus of diaphragm to duodenjejunal flexure
#20 Airway: if altered mental status
Breathinf: assess oxygenatn and ventilatn
Circulation: identif signs of shock(tachycar,hotn,agitation)
Disability: evaluate mental status


























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








