
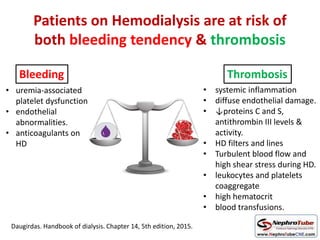
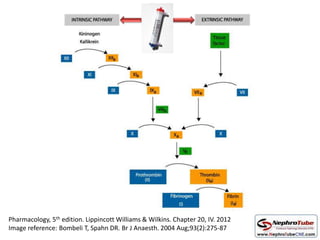
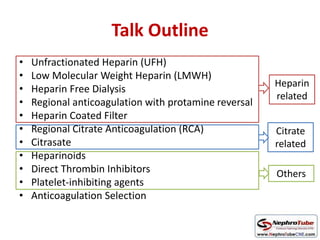
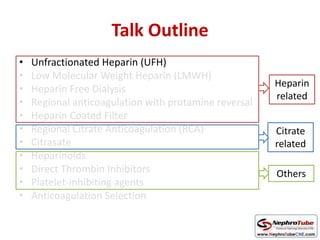
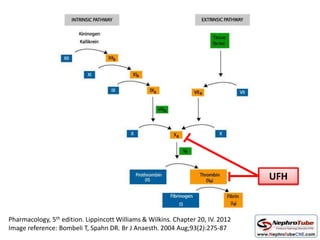

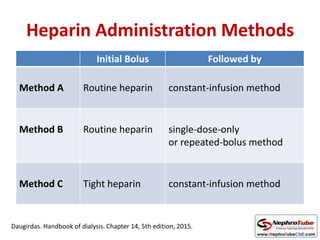
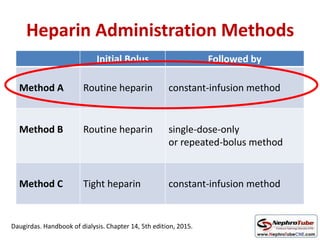
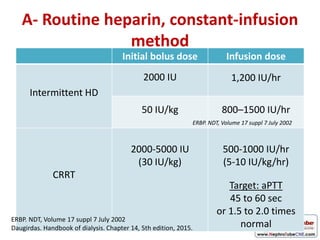
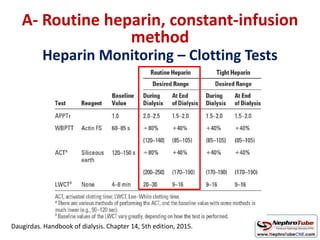
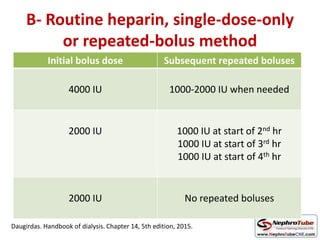
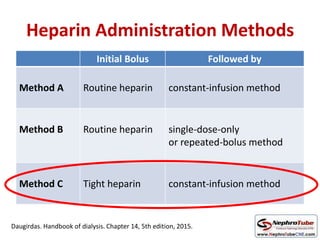
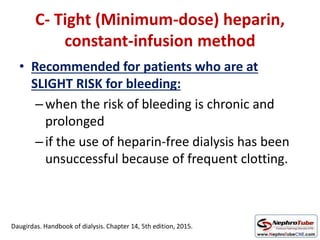
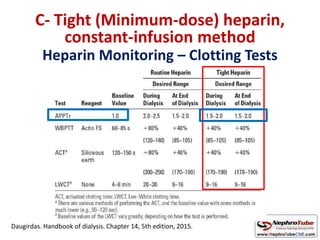
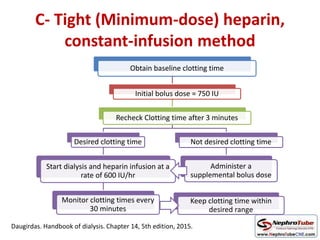
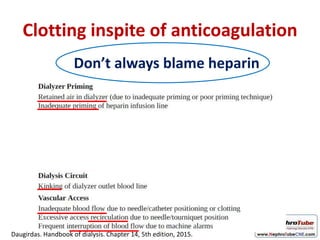
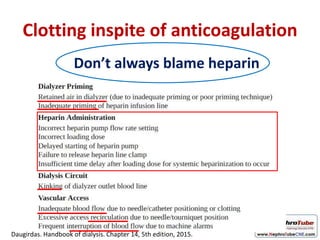
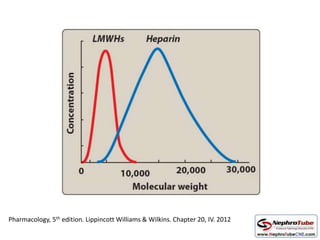
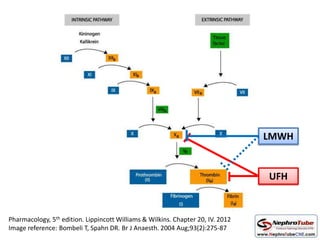
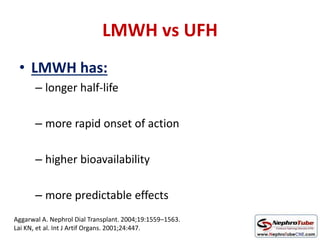
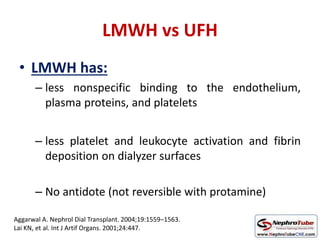
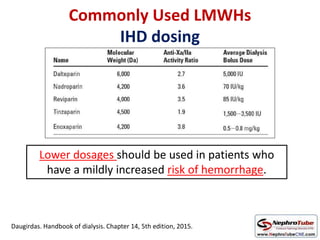
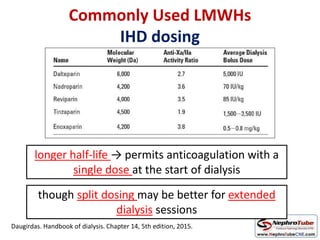
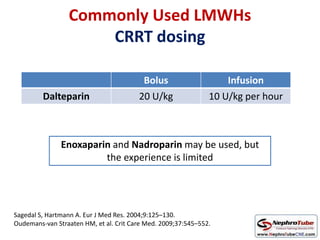
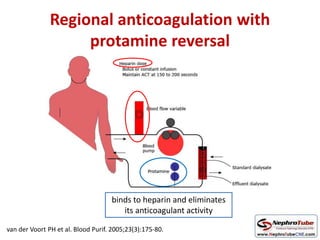
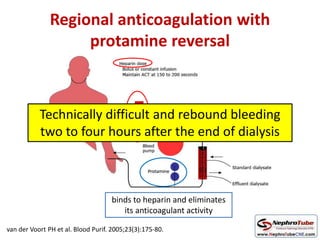


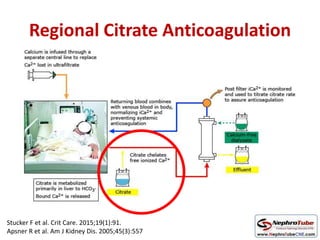
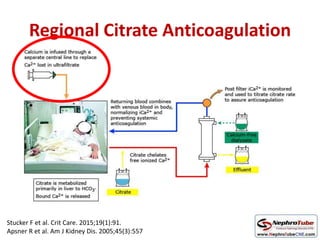
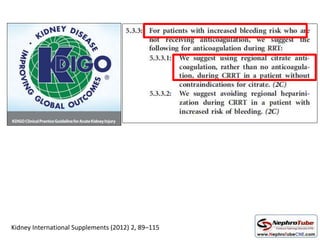
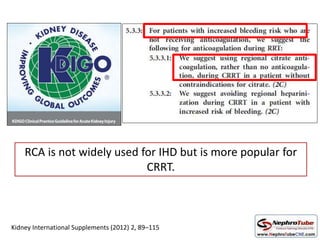
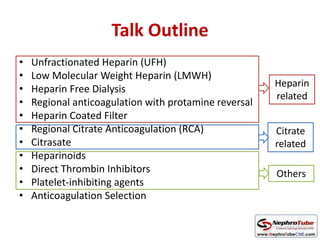
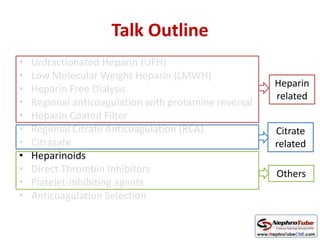
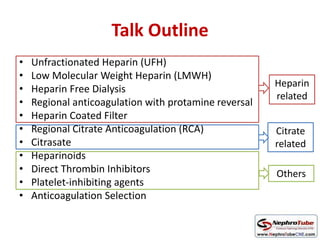
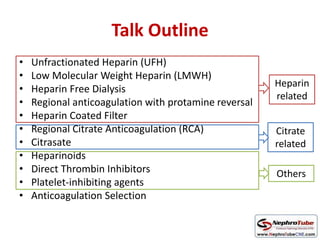
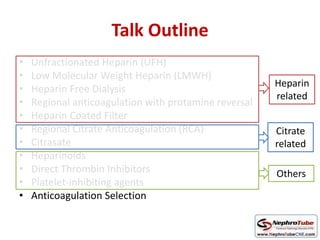
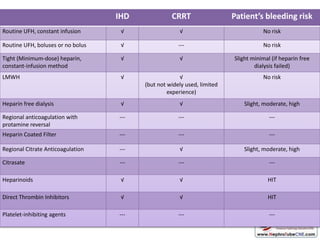


This document discusses various protocols for anticoagulation during hemodialysis. It begins by noting that patients on hemodialysis are at risk of both bleeding and thrombosis. It then outlines several protocols for anticoagulation including unfractionated heparin (UFH) administered via constant infusion or intermittent bolus, and low molecular weight heparin (LMWH). LMWH has benefits over UFH like longer half-life and more predictable effects, but is also more expensive. The document also discusses heparin-free dialysis, regional citrate anticoagulation, and other alternatives to standard heparin protocols. Selection of the optimal anticoagulation method requires consideration of individual patient




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











