Downloaded 272 times

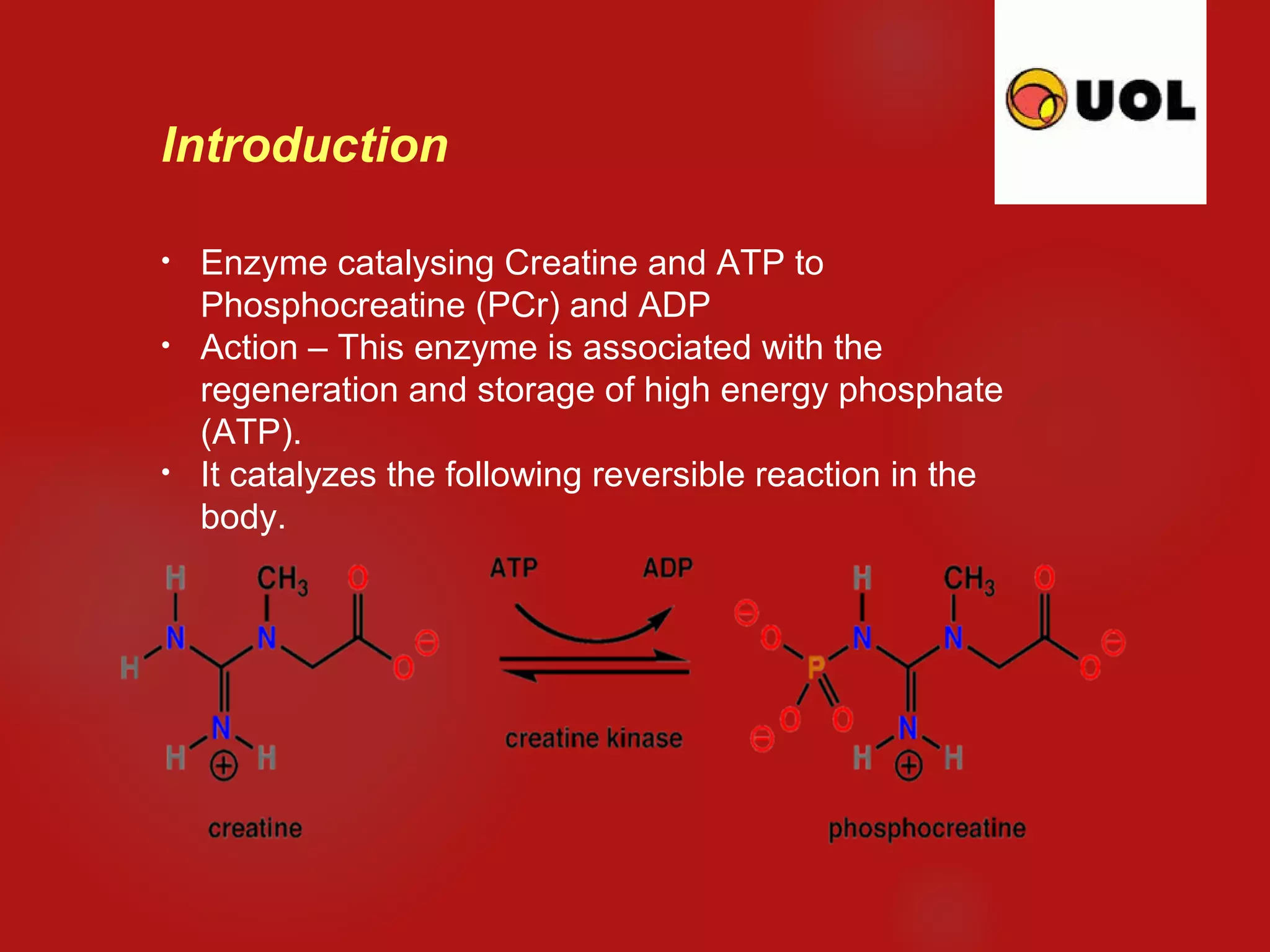













This document discusses creatine kinase (CK), an enzyme that plays an important role in energy metabolism. It has three isoenzymes - CK-MM found mainly in skeletal muscle, CK-MB found in heart muscle, and CK-BB found primarily in brain and smooth muscles. CK levels are measured to diagnose conditions like heart attack, muscle damage, and brain injury. An elevated CK level suggests muscle or tissue damage, with each isoenzyme rising in response to damage in its specific tissues. The test is also used to monitor muscle diseases and can be affected by exercise, medications, toxins, and other clinical factors.


























































































