• TESTS OFBIOCHEMICAL ACTIVITY
• Transaminases
• The two enzymes which are sensitive indicators of hepatocellular
damage, are:
• Aspartate aminotransferase or glutamic oxaloacetate transaminase (AST
or GOT) Normal range: 10-40 u/L
• Alanine aminotransferase or glutamic pyru-vate transaminase (ALT or
GPT). Normal range: 7-56u/l
• They are released into the circulation by hepatocellular necrosis.
• AST is a mitochondrial and cytosolic enzyme present not only in the
liver, but also in the heart, skeletal muscle, brain, pancreas, lung,
red blood cells and kidney. Hence, whenever these tissues are acutely
damaged,AST will be increased.It has a long serum half life 48 hours
5.
• ALT isa cytosolic enzyme seen mainly in hepa-tocytes. It has a shorter half-life of
18 hours.
• Hence an increased ALT is more specific and sensitive for hepatocellular injury than
AST.
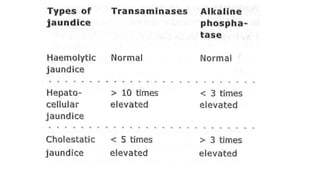
• In acute hepatitis, the transaminases are 10 times above normal.
• In cholestatic jaundice, they are about 5 times above normal.
• Very high levels may be seen in drug-induced hepatitis, especially that due to
paracetamol.
• In chronic hepatitis, the levels are around 5 times above normal
• AST is relatively more specific for chronic liver disease and alcoholic liver
disease and ALT for acute liver disease. ( in chronic liver disease low grade
ongoing inflammation,rate of cell death is slow,liver adaptation)
• In chronic liver disease progressive mitochondrial damage ,its levels rise more
6.
• Reduced perfusionof the liver in congestive cardiac failure leads to hypoxia, a
potent cause of leakage of enzymes from the cells. Hence, tran-saminases may
be elevated in CCF. Here, the patient develops hepatocellular jaundice and
tender hepatomegaly, which may be mistaken as viral hepatitis. This condition is
called ischaemic hepatitis.
• Similarly, haemodynamic changes like loss of fluid due to diarrhoea and
vomiting, may lead to small transient elevations of transaminases, which may
confuse the clinician. ( hypovemia-reduced b.flow to liver and skeletal
muscles- ischemia- elevated transaminases)
• Unexpectedly elevated aminotransferase may be seen in:
• Obesity. (Excess fat in hepatocyte- injury)
• Diabetes mellitus.
• Alpha-1 antitrypsin deficiency.
• Asymptomatic chronic hepatitis B and C.
• Wilson's disease
7.
• Diagnostic valueof transaminases
• In hepatitis, elevation of transaminases precedes that of serum bilirubin by
about one week. ( hepatocytes damaged –release into blood stream , bilirubin
accumulates only when liver dysfunction progress far enough to effect
uptake,conjugation,excretion of bile -more complex and resilient process)
• Maximum levels of transaminases are seen in conditions causing extensive
hepatocellu-lar necrosis like drug-índuced hepatitis, viral hepatitis, ischaemic
hepatitis, and toxic hepatitis due to carbon tetrachloride and poisonous
mushrooms (Amanita phalloides).
• De Riti's ratio: In alcoholic hepatitis, the SGOT: SGPT ratio is always 2:1. The
ratio is usually less than 1 in patients with acute and chronic non-alcoholic
hepatitis. This may be useful in adolescents who may present with alchohalic
hepatitis
• In alchohalic hepatitis AST is raised than ALT due to alchohal toxic to
mitochondria- leads to hepatocyte injury
8.
• TESTS OFCHOLESTASIS
• Alkaline Phosphatase (AP) adults : 40-130u/l ,children/teens: up to 350u/l
• Serum alkaline phosphatase activity actually refers to a group of isoenzymes that hydrolyze
organic phosphate esters at alkaline pH, generating inorganic phosphate and an organic
radical.
• In the liver, AP is synthesized by the canalicular membrane of the hepatocytes and
excreted with bile into intestine
• Mechanisms contribute to the raised levels of AP
• Regurgitation
In cholestatic jaundice, AP is regurgitated into the plasma from the hepatocytes and can be
differentiated from other AP by electrophoresis. It is called 'fast AP', because of its rapid
mobility.
• Increased synthesis
Local or diffuse cholestasis induces the synthesis of AP by the biliary canaliculi, which
regurgitates into the plasma.
Raised AP is a sensitive indicator of cholestasis, whether intrahepatic or extrahepatic. Its levels
are higher in children with posthepatic obstruction like biliary atresia, than in neonatal hepatitis.
9.
Dissociated jaundice
• Inincomplete biliary obstruction or when intra-hepatic
obstruction is only partial, bilirubin may be normal or only
slightly elevated, while alkaline phosphatase is quite high. This
is seen in space-occupying lesions like metastasis
• ( Bile cannot flow freely-congestion in bileducts leading to
increased ALP levels- due to bileduct damage and cholestasis
Bilirubin processing and excretion are still functioning to some
degree is normal / slightly increased in partial obstruction )
10.
Sources of alkalinephosphatase
• Liver-canalicular membrane.
• Bone—osteoblasts.
• Leukocytes.
• Small intestine—brush border of the entero-cytes.
• Kidney-proximal convoluted tubules.
• Placenta.
• The intestinal AP may be elevated in cirrhosis( overproduction AP
isozymes /often result in cross reactivity –altered syn of intestinal AP ), but
not in intestinal diseases.
• The bone isoenzyme is high in growing children. It is also increased in rickets,
osteomalacia and osteogenic deposits in bone
• Zinc is a cofactor for AP and in any condition causing zinc defeciency,AP may
be reduced
11.
• Diagnostic Valueof Alkaline Phosphatase
• Serum AP is elevated in the following conditions:
• It is elevated 5 times above normal in cholestasis, both intrahepatic and
extrahepatic.
• There is no difference in the level in extrahepatic cholestasis due to
biliary atresia, sclerosing cholangitis, bile duct strictures or cancer.
Values are similarly increased in patients with intrahepatic cholestasis
due to neonatal hepatitis, drugs, . It is not possible to differentiate
extrahepatic cholestasis from intrahepatic cholestasis based on AP
levels
• Normal level is 100iU/litre
13.
• The mostpractical method to decide whether a high serum AP is due to liver disease is
by measuring another enzyme that rises in cholestatic disease and that is more specific
to the liver is GGT or 5-nucleotidase
• Gammaglutamyl Transpeptidase (trans-ferase)
• GGT is synthesized by the epithelium of the small bile ductules and hepatocytes.
• It is also present in other tissues like
• pancreas
• kidney
• spleen
• brain
• heart
• seminal vesicles.
• How-ever, elevated levels are found in disorders of liver, biliary tract and pancreas.
• This is one of the most sensitive tests for the presence of hepatobiliary disease.
• GGT levels are higher in biliary tract disease and cholestasis than in hepatocellular
disease.
14.
• The followingdrugs may elevate GGT levels.
1. Anticonvulsants like phenytoin sodium, barbiturates and valproic acid.
2. Tricyclic antidepressants.
3. Analgesics.
4. Anticoagulants like warfarin.
5. Antihyperlipidaemics.
6. Oral contraceptive pills.
• GGT does not help to differentiate ex-trahepatic from intrahepatic
cholestasis.
• The cholestatic jaundice with normal GGT are are
1. Progressive familial intrahepatic cholestatis (type 1 byler disease)
2. Type 2 byler disease
3. Benign recurrent intrahepatic cholestasis
16.
• 5-Nucleotidase
• Thisenzyme is found in liver, intestine, heart, blood vessels and endocrine pancreas.
• In the liver this enzyme is located in both sinusoidal and canalicular plasma membranes.
• elevated in hepatobiliary disease (along with AP is of hepatic origin)
• Leucine Aminopeptidase
• This is found in all human tissues , with high activity in the liver, where it is located in the
biliary epithelium.
• values are highest in biliary obstruction.
• Serum bilirubin
• Total bilirubin- 0.3 – 1.2 mg/dL
• Unconjugated (Indirect)- 0.2 – 0.8 mg/dL
• Conjugated (Direct)- 0.1 – 0.3 mg/dL
• Normal pathway
• Heme Biliverdin
→ → Unconjugated Bilirubin (indirect) (Liver)
→ → Conjugated
Bilirubin (direct) (Bile)
→ → Intestine → Urobilinogen →→ Urobilin (urine) +
Stercobilin (feces)
17.
• Many laboratoriesstill use spectrophotometry to measure serum bilirubin as direct or
indirect fractions. This fractionation is based on the original van den Bergh reaction. In this
reaction, bilirubin reacts with Ehrlich's diazotized sulfanilic acid, to produce
chromogenic compounds that can be detected colorimetrically.
• Direct van den Bergh Reaction
• reaction is carried out in an aqueous medium. The water-soluble conjugated bilirubin reacts
to give the direct reaction.
• Indirect van den Bergh Reaction
• The reaction is carried out in methanal.
• The intramolecular hydrogen bonds of unconju-gated bilirubin are broken thus, both
conjugated and unconjugated bilirubin react, giving a measure of the total bilirubin level.
• The total minus direct-reacting bilirubin gives the indirect value, which is a measure of
unconjugated bilirubin level.
• Urine bilirubin: cholestatic jaundice bilirubin is excreted in urine
• Urine urobilinogen: increased in hepatitis, cirrhosis, haemolytic anemia, severe
constipation
• Absent in complete biliary obstruction , severe diarrhea,
prolonged antimicrobial therapy
20.
Tests of liversynthetic function
• The normal serum albumin is about 3.5-5 g%.
• It is synthesized only in the smooth endoplasmic reticulum of the hepatocytes at the rate of 150 mg/kg/day in children.
• The normal adult liver produces about 10 g albumin daily, whereas a cir-rhotic liver can produce only about 4 g/day.
• In liver disease, the fall in serum albumin concentration is slow, as the half-life of albumin is about 22 days. Hence, a low
serum albumin is taken as a sign of chronic liver disease rather than acute disease.
• A patient with fulminant hepatitis may die with a virtually normal serum albumin value while a patient with decompensated
cirrhosis may have a low serum albumin. ( due to longer halflife)
• Serum Globulins
• Serum immunoglobulins are produced by stimulated B-lymphocytes and hence they do not directly test liver function. In
chronic liver disease, the function of the reticuloendothelial cells of the liver is impaired. Hence bacteria cannot be destroyed
and they reach the circulation, stimulating the B-lymphocytes to produce immunoglo-bulins.
• Serum globulins can be separated into four:
• Alpha-1 globulin- this consists of caeruloplas-min, alpha-lantitrypsin and orosomucoid, all of which are acute phase
reactants and are increased in any type of inflammation.
• Alpha-2 globulin-haptoglobin, which is also an acute phase reactant.
• Beta globulin— transferrin and beta lipoprotein.
• Gamma globulin-IgG, IgM and IgA, which are synthesized in the reticuloendothelial system by plasma cells
• The gamma globulin level is increased in cirrhosis due to increased production. The increased number of plasma cells in the
bone marrow may be the source.
• Persistant hypergammaglobulinemia is also seen in autoimmune chronic hepatitis
21.
Tests of liverfunction tests
• Elevation of Specific Immunoglobulins
• IgG: increase in chronic active hepatitis and cryptogenic cirrhosis. In viral hepatitis there is a slow and sustained increase.
• IgM: increased in primary biliary cirrhosis and to a lesser extent in chronic active hepatitis and cryptogenic cirrhosis.
• IgA: increased in alcoholic cirrhosis and to some extent in cryptogenic cirrhosis and primary biliary cirrhosis.
• Bile Acids
• The liver is the only organ that can synthesize bile acids. About 250-500 mg is synthesized and lost in the stools daily
• The primary bile acids, cholic acid and cheno-deoxycholic acid, are formed from cholesterol.
• The colonic bacteria convert the primary bile acids to the secondary bile acids, mainly deoxycholic acid and a very little lithocholic
acid, by 7- alpha-dehydroxylation.
• Tertiary bile acids like ursodeoxycholic acid are produced in the liver by epimerization of the secondary bile acids.
• The bile acids are conjugated in the liver with the amino acids glycine and taurine. This prevents reabsorption in the biliary tree and
small intestine but permits conservation by absorption in the terminal ileum
• Bacteria can hydrolyze bile salts to bile acids and glycine or taurine.
• The absorbed bile salts enter the portal venous system and reach the liver where they are taken up actively by the hepatocytes. The
bile salts are reconjugated and excreted in the bile. This enterohepatic transport of bile salts takes place 2-15 times per day, which
helps to prevent the loss of bile salts. The maintenance of normal serum bile acids depends on the hepatic blood flow, hepatic
uptake, secretion of bile acids by the liver and enterohepatic circulation.
• Serum Bile Acids can be Determined by Three Methods
• Gas-liquid chromatography.
• Enzymatic assays.
• Radioimmunoassay.
22.
• Pathway ofBile Acids and Bile Salts
• A. Bile Acid Synthesis (Liver)
• 1. Starts from cholesterol
• 2. Two main primary bile acids:
• • Cholic acid (trihydroxy)
• • Chenodeoxycholic acid (dihydroxy)
•
B. Conjugation (Still in Liver)
• 3. Conjugated with:
• • Glycine or Taurine
• 4. Forms bile salts:
• • E.g., Glycocholic acid, Taurocholic acid
•
C. Secretion and Action
• 5. Stored in the gallbladder, released into duodenum after meals
• 6. Bile salts emulsify dietary fats
•
D. Enterohepatic Circulation
• 7. 95% reabsorbed in the ileum, returned to the liver via the portal vein
• 8. 5% lost in feces — liver synthesizes new bile acids to replace
•
E. Bacterial Modification in Colon
• 9. Gut bacteria deconjugate and dehydroxylate bile salts:
• • Form secondary bile acids:
• • Deoxycholic acid (from cholic acid)
• • Lithocholic acid (from chenodeoxycholic acid)
• . Some secondary bile acids are reabsorbed, sent back to liver, and can be reconjugated
23.
• Elevated serumbile acid levels are specific for hepatobiliary disease
• Serum bile acids are normal in Gilbert's syn-drome.
• In cholestasis, the ratio of serum trihydroxy to dihydroxy bile acids
increases.
• In hepatocellular failure, the ratio decreases, the main bile acid being
chenodeoxycholic acid.
• The sensitivity of serum bile acid estimation is less for detecting
the hepa-tocellular damage( mild- moderate) in viral hepatitis or
chronic liver disease.
24.
• Prothrombin Time(Quick's one-stage prothrombin time)
• Liver helps in the Production of all the clotting factors except von Willebrand’s factor( megakaryocytes
and vascular endothelial cells.)
• Factors II, VII, IX and X require vitamin K for their activation and are hence called vitamin K
dependent factors. Vitamin K is essential for the gamma carboxylation of glutamic acid residues in
their amino terminal regions.
• The carboxylation enzyme system is localized to the hepatocyte microsomes. As the damaged
hepatocytes are unable to do this, the vitamin K dependent factors cannot be carboxylated and are
thus non-functional. Therefore, they cannot take part in the coagulation cascade, resulting in bleeding
manifestations.
• Normal values are 12-13 seconds.
• Prolongation of more than 2 seconds is considered pathologic;
• values more than 3 seconds above normal indicate a risk of bleeding.
• prolonged prothrombin time may be seen in hepatocellular jaundice and in cholestatic jaundice.
• If the prothrombin time becomes normal after vitamin K injection, the patient has cholestatic
jaundice, while in severe hepatocellular jaundice the prothrombin time remains prolonged
• Prolonged PT is also seen in non hepatic causes like DIC .factor viii levels may help to differentiate
haemorrhage due to severe liver disease (normal factor viii levels) from DIC ( decreased factor viii
levels)
25.
• International NormalizationRatio (INR)
• This system standardizes the PT for different thromboplastin reagents, thus providing a
universal standard by which to compare any given laboratory's result with that of the WHO
stan-dard. The INR is calculated as follows:
• INR= (Patient's PT/normal PT) ISI
• Normal PT = Mean PT of the target population in seconds
• Liver biopsy is contraindicated if INR is > 1.3. INR helps to monitor patients on warfarin
therapy.
• Uses of PT
• helps to differentiate cholestatic jaundice from hepatocellular jaundice
• It is of high prognostic value especially in acute hepatocellular disease (prolonged PT 5-6
seconds of normal value)
• A prolonged PT is not specific for liver disease as it may be seen prolonged PT levels in
• congenital deficiency of coagulation factors
• acquired conditions like DIC and ingestion of
drugs( warfarin,cefalosporins,INH,MTX, valproate) that affect the prothrombin
complex.
26.
• Partial ThromboplastinTime (PTT)
• This measures the generation of thrombin by the intrinsic pathway, which uses all the clotting factors
including factors IX (vitamin K depen-dent) and VIII (with the exception of factor VII).
• Thrombin Time
• The normal hepatocytes remove sialic acid residues from fibrinogen. Hence, in hepatocellular
damage, this function is decreased and fibrinogen molecules develop excessive sialic acid
• These altered fibrinogen molecules are dysfunctional and cannot function properly. This
contributes to the haemorrhagic diathesis of liver disease.
• The thrombin time is tested by adding thrombin to citrated plasma and measuring the time for clot
formation. This test is sensitive to the levels of fibrinogen.
• The abnormal fibrinogen with excess sialic acid produced in liver damage may not
polymerize properly when cleaved to fibrin monomer and hence the TT is prolonged
• Summary of Coagulation Abnormalities in Liver Disease
1. Bleeding time— increased or normal.
2. Prothrombin time and PTT- increased.
3. Thrombin time-increased or normal.
4. Factor VIII and Fibrinogen-increased or normal.
5. Factors II, V, VI, IX, X; antithrombin III and plasminogen-Decreased.
6. Fibrin degradation products-increased or normal.
7. Dysfibrinogenaemia.
27.
• Ammonia
• producedmainly in the colon by the action of bacterial urease on dietary proteins and amino acids.
• Ammonia is converted by the liver into urea by the Krebs-Henseleit urea cycle and into glutamine.
• The liver normally removes 80% of the portal venous ammonia in a single pass.
• In chronic liver disease and portal hypertension, large amounts of ammonia bypass the liver and
reach the brain, contributing to encephalopathy
• Plasma and urine aminoacids
• Elevated levels of methionine, phenyl alanine and tyrosine may be seen in patients with significant
hepatocellular disease of any cause as well as in specific hereditary disorders like:
1. Wilson's disease. ( kf rings, neuropsychiatric symptoms)
2. Galactosaemia.( oildroplet cataracts, vomiting jaundice,e.coli sepsis)
3. Hereditary fructose intolerance.( hypoycemia,vomiting,lethargy, hepatomegaly after fruit )
• Serum lipids and lipoproteins
• Lipids and lipoproteins are mainly synthesized in the liver, except chylomicrons, which are synthesized in the
intestine
• Lipids in Cholestatic Jaundice
• Serum cholesterol (normal <200mg/dl) is increased in cholestatic jaundice.Skin xanthomas develop if the
level is 5 times above normal.
• An abnormal lipoprotein, viz, lipoprotein-X is synthesized in biliary atresia and neonatal hepatitis. Following
cholestyramine therapy, the level decreases in NH, whereas it continues to be high in BA.
28.
Tests of
quantitative
functions
• Teststhat measure haemodynamic status of the liver. Serial estimates of
quantitative liver function in the early stages would be helpful both in monitoring
treatment and in prognosis. But they are not important in diagnosis.
• These tests are very complex and are done only in research laboratories.
• Galactose elimination test.
• Breath tests.
• Monoethylglycinexylidide test (MEGX test).
• Galactose Elimination Test
• Galactose is taken up by the liver and converted to galactose-1-PO by
galactokinase, which is the rate limiting reaction in galactose elimination from the
blood.
• Galactokinase activity depends upon the functional liver mass. galactose
elimination gives an estimate of the functional hepatic cell mass.
• Breath Test
• Aminopyrine labeled with C14 is given orally. It is metabolized by cytochrome P-
450 dependent demethylation to carbon dioxide.
• This demythylation occurs only in the liver. Samples of "CO2 are collected from
the mouth for 2 hours.
• The test tells about residual functional microsomal mass and viable hepatic
tissue.
29.
Tests of
quantitative
functions
• ReducedN-demethylation is due to loss of liver cell volume.
• This test is useful in the prognosis and to assess therapy. It may be useful to assess
the effect of drugs on the hepatic microsomal enzyme function
• It is not useful for screening or diagnosis
• Monoethylglycinexylidide FormationTest (MEGX test)
• Lignocaine clearance is decreased in liver disease and lignocaine clearance is a
useful quantitative liver function test. MEGX is the main metabolite of lignocaine.
• It is formed in the hepatocyte microsomes by cytochrome P450-dependent
demethylation.
• Lignocaine is given intravenously and serum MEGX is measured at 15 minutes and
30 min-utes. It diffuses out of the hepatocytes where it is formed, into the
bloodstream, where it can be measured.
• levels are decreased in cirrhosis
• MEGX test is also useful to assess the quality of organ donors. Low donor
MEGX formation is significantly correlated with poor graft survival in the
recipient.
Radiology
• Ultrasonography
• Ultrasonographyof abdomen provides information on the size of liver, spleen,
pancreas, kidneys and gall bladder.
• It detects gallstones and tumours, haemangiomas, abscess and cysts within
the liver. It allows targeting of lesions for liver biopsy.
1. A small or absent gall bladder after fasting suggests either severe
intrahepatic cholestasis or biliary atresia in the neonate.
2. Extra-hepatic bile ducts are usually identified but intrahepatic bile ducts are not
seen unless dilated, secondary to biliary obstruction.
3. Dilated intrahepatic bileducts are not seen in extrahepatic biliary atresia in
the neonate.
• CT scan
• CT scan is very useful for the detection and biopsy of hepatic tumours and space-
occupying lesions.
• Intravenous contrast medium causes enhancement of vascular lesions and the
wall of abscesses, and helps in the differentiation of tumours from other solid
masses.
• CT Angiography allows non invasive evaluation of vascular structures
CT scan of brain helps to detect cerebral oedema in fulminant hepatic failure and
helps in the diagnosis of metabolic liver diseases like Wilson’s disease
( hypodensities in basal ganglia in puts men and globes pallidus)
33.
Radiology
• Endoscopic RetrogradeCholangiopancreatography (ERCP)
• Here, a fibre-optic duodenoscope is passed into the first part of duodenum, the ampulla of Vater is identified, the pancreatic and biliary
ducts are cannulated, and contrast is injected.
• This is very useful in the evaluation of extrahepatic biliary disease in older children like choledochal cysts, primary sclerosing
cholangitis and chronic pan-creatitis. It is technically very difficult in neonatal cholestasis.
• It can also be used to remove common bile duct stones and for insertion of biliary stents.
• Percutaneous Transhepatic Cholangiog-raphy (PTC)
• This technique is useful for the identification of biliary disease if intrahepatic bile ducts are dilated secondary to obstruction
• A thin needle (Chiba needle) is passed through the liver. The bile ducts or gall bladder are punctured and radiological contrast is injected.
• External drainage of the biliary tree, dilatation of biliary strictures and the insertion of biliary stents are all possible using this
technique
• Angiography
• Visualization of the coeliac axis, and hepatic and splenic blood vessels, is obtained by femoral artery catheterization and injection of
radiological contrast..
• This technique has two parts:
• • The arterial phase, which provides information on the coeliac axis, hepatic and splenic artery abnormalities, vascularization
and anatomy of hepatic tumours, hepatic haeman-giomas or detection of hepatic artery thrombosis
• • The venous phase, which provides information about the patency of the portal, splenic and superior mesenteric veins and the
presence of portal hypertension by identification of mesenteric, oesophageal or gastric varices. In skilled hands the
investigation can be performed in infants, with little risk
• Hepatic artery embolization is now indicated for the treatment of hepatic haemangiomas or in the control of liver haemorrhage from
trauma or needle biopsy. Angioplasty for portal or hepatic vein obstruction is also feasible using angiographic techniques.
34.
Radiology
• Magnetic ResonanceImaging (MRI)
• MRI scanning has now replaced hepatic angiography as the best way to stage or diagnose hepatic
tumours and identify their vascular supply.
• It may provide valuable information about liver or brain consistency and storage of heavy
metals, for example, iron in haemochromatosis, and copper in Wilson's disease and cerebral
oedema in acute liver failure.
• The recent development of MRI cholangio-pancreatography (MRCP), in which
abnormalities of both intra- and extrahepatic biliary ducts, and also the pancreatic duct
may be detected may replace ERCP as a diagnostic investigation.
35.
Liver biopsy
• Indications
•Unexplained hepatomegaly
• Unexplained jaundice
• Unexplained elevation of liver enzymes
• Cholestatic liver disease-biliary atresia and neonatal hepatitis
• Cirrhosis
• Chronic hepatitis
• Drug-related hepatitis
• Infections of liver like tuberculosis
• Enzyme analysis for inborn errors of metabolism
• Copper estimation in Wilson's disease when all other tests are equivocal
• Storage diseases
• Grading and staging of non-alcoholic steato-hepatitis
• Post liver transplantation to assess acute rejection
• It is important to know about the size and consistency of the liver, and the
presence of cysts or dilated bile ducts by ultrasound.
• It is helpful to mark a spot on the abdomen by USG to ensure an accurate biopsy.
• Prothrombin time should be within 3 seconds of control values; platelet
count should be >60,000.
• Biopsy specimens should be obtained for routine histopathology, microbiology,
electron micros-copy, immunohistochemistry, and copper (if ap-propriate), and
frozen in liquid nitrogen for enzymatic or metabolic investigations.
• . Adequate monitoring of vital signs post-biopsy is essential to detect
complications such as haemorrhage
36.
• Contraindications ofLiver Biopsy
Prothrombin time > 3 seconds prolonged or
INR> 1.3
Thrombocytopenia-platelet count < 60,000
Presence of grossly dilated bile ducts
Angiomatous malformation of the liver
Hydatid cysts:
Severe ascites
Uncooperative patients
• Liver biopsy can be performed by three routes:
• Percutaneous route: transthoracic/subcostal.
• Transvenous route (trans jugular approach)
• By laparoscopy