Downloaded 54 times







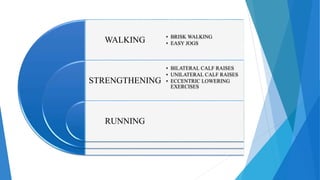
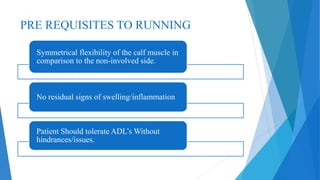




Tennis leg, or rupture of the medial head of the gastrocnemius muscle, is commonly seen in tennis players and other athletes involving running and jumping. It occurs due to forced dorsiflexion of the ankle while the knee is extended. Clinically, it presents with a sudden "pop" in the calf followed by pain and swelling. Treatment involves RICE initially followed by rehabilitation depending on the grade of tear, ranging from stretching and strengthening exercises for grade 1, to immobilization and surgery for grade 3 tears. Proper rehabilitation is important to prevent recurrence and allow a full return to activity.



































































