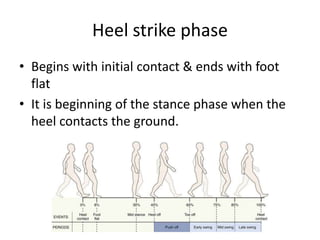
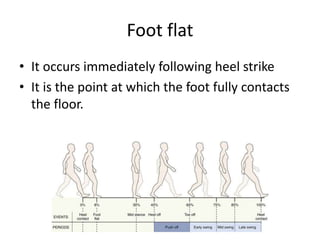
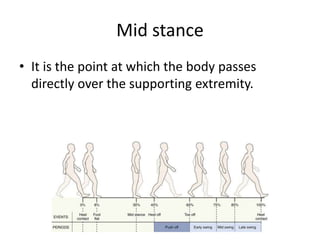
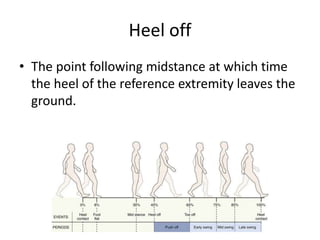
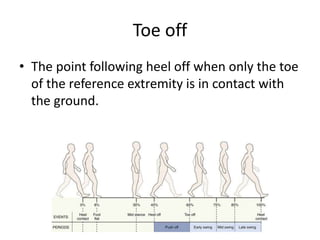
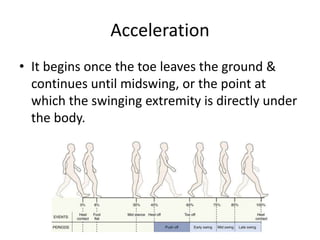
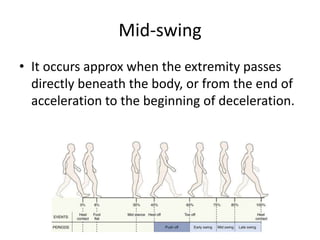
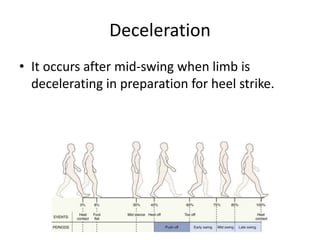
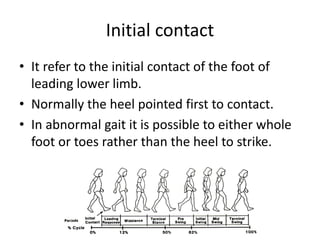
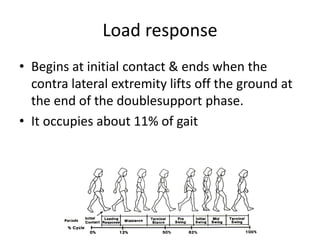
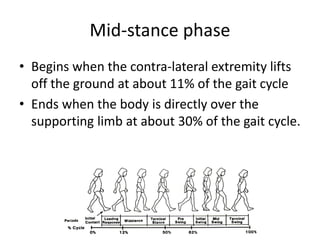
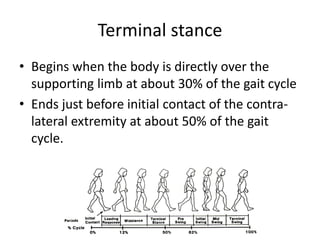
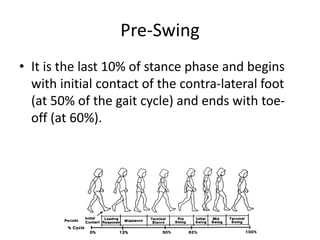
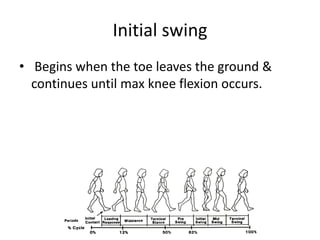
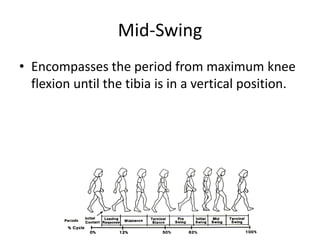
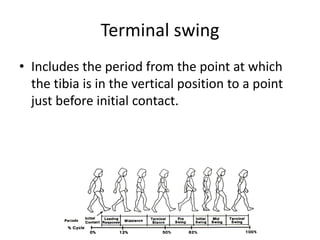
This document describes the normal gait cycle and phases of gait, including stance and swing phases. It also discusses various temporal and distance gait variables that are used to analyze walking, such as stride length, step length, cadence, and velocity. Additionally, it outlines several types of abnormal pathological gaits that can result from different medical conditions, such as antalgic, psoatic, hemiplegic, cerebellar ataxic, and Parkinsonian festinating gaits.

























![Posture- Physical Therapy [VNSGU]](https://cdn.slidesharecdn.com/ss_thumbnails/posture-180915145350-thumbnail.jpg?width=640&height=640&fit=bounds)





























































