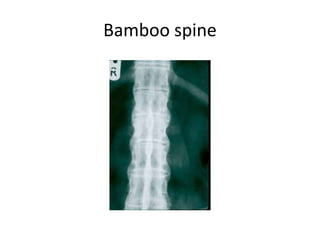
Ankylosing spondylitis is a chronic inflammatory disease characterized by inflammation of the spine and sacroiliac joints that commonly affects the axial skeleton. It is strongly associated with the HLA-B27 gene and causes new bone formation that can result in fusion of the vertebrae and loss of spinal mobility. Physical therapy aims to maintain flexibility while NSAIDs and COX-2 inhibitors are first-line treatments for pain and stiffness. Surgical options may include spine stabilization for fractures or osteotomies to correct spinal deformities.