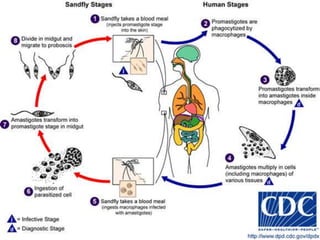
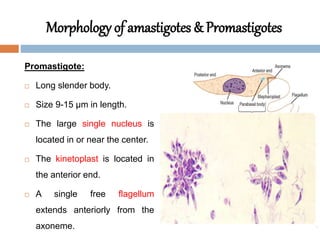
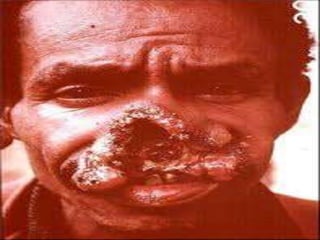
Leishmania species are protozoan parasites that cause leishmaniasis. They are transmitted through the bite of infected sand flies. The life cycle involves promastigotes that develop in the sand fly gut and amastigotes that multiply within human macrophages. Leishmaniasis exists in visceral, cutaneous, and muco-cutaneous forms depending on the infecting species and affected tissues. Diagnosis involves identifying amastigotes in tissue samples through microscopy or culturing. Control relies on reducing reservoir hosts and applying preventative measures against sand fly bites.