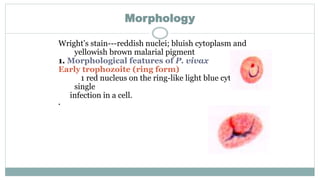
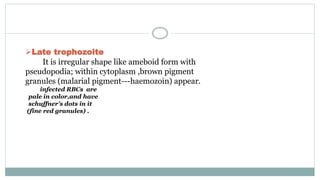
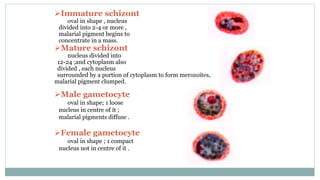
This document provides information about Plasmodium vivax, the parasite that causes benign tertian malaria. P. vivax originated in Asia and is mostly found in Asia, Latin America, and parts of Africa. It has dormant liver stages called hypnozoites that can activate months or years later to cause relapse. Symptoms include fever, chills, sweats, abdominal pain, nausea and vomiting. Diagnosis involves blood film examination, rapid tests, culture and PCR. Treatment includes chloroquine and primaquine which target the blood and liver stages respectively. Prevention involves chemoprophylaxis with drugs like chloroquine and mosquito control measures.