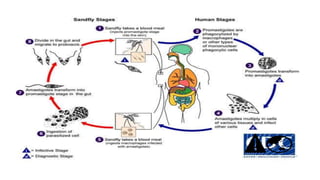
This document provides information on Leishmania donovani, the parasite that causes visceral leishmaniasis or kala-azar. It discusses the history and classification of L. donovani, its life cycle between human and sandfly hosts, clinical symptoms of kala-azar including fever and spleen/liver enlargement, and methods for laboratory diagnosis and treatment/prevention.












![Trypanosoma [1]](https://cdn.slidesharecdn.com/ss_thumbnails/trypanosomaseminar1-170312074241-thumbnail.jpg?width=640&height=640&fit=bounds)








































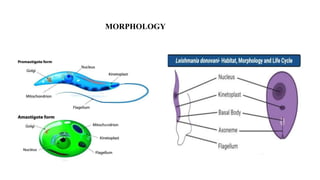
![Genus_Leishmania_new_lecture[Autosaved].ppt_2 - Copy.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/genusleishmanianewlectureautosaved-250720135838-6fd1097a-thumbnail.jpg?width=640&height=640&fit=bounds)



































