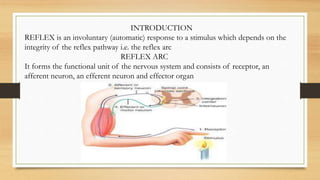
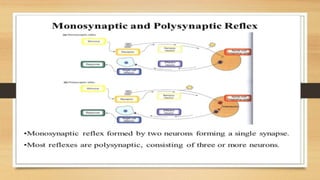
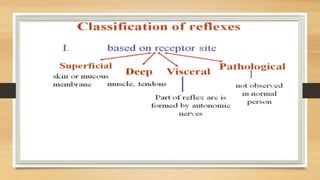
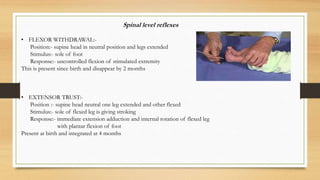
The document discusses reflexes as involuntary responses to stimuli, detailing the anatomy of reflex arcs, and their classifications into monosynaptic and polysynaptic types. It also covers various specific reflex tests, including the biceps, triceps, patellar, and Achilles reflexes, along with their neurological significance and the implications of absent or exaggerated reflexes. Additionally, it explains primitive reflexes observed in infants, their importance for motor development, and the stages at which they are integrated.