Anatomy of Brachial Plexus (by Murtaza Syed AKUH Karachi)
•Download as PPT, PDF•
78 likes•19,450 views

The brachial plexus is a network of nerves in the neck, axilla, and arm that originates from the cervical and thoracic spinal nerve roots. It provides motor and sensory innervation to the upper limb. Specifically, the brachial plexus forms from the ventral rami of cervical nerve roots C5-C8 and thoracic nerve root T1. These rami come together to form the roots, trunks, divisions, cords, and peripheral branches that make up the brachial plexus and allow it to innervate the muscles and skin of the arm.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anatomy of Brachial Plexus (by Murtaza Syed AKUH Karachi)
Similar to Anatomy of Brachial Plexus (by Murtaza Syed AKUH Karachi) (20)
More from Murtaza Syed
More from Murtaza Syed (20)
Recently uploaded
Recently uploaded (20)
Anatomy of Brachial Plexus (by Murtaza Syed AKUH Karachi)
- 1. BRACHIAL PLEXUS • By: Syed Irshad Murtaza • Technologist CNPS AKUH Karachi • Date: 13-05-2014
- 2. What is the Brachial Plexus? • Introduction • A network of spinal nerves that originates in the back of the neck, extends through the axilla (armpit) and gives rise to nerves to the upper limb. • The brachial plexus is a network of nerve fibers, running from the spine, formed by the ventral (Anterior) rami of the lower four cervical and first thoracic nerve roots (C5-C8, T1).
- 5. Anatomy • Brachial Plexus proceeds through the neck, the axilla (armpit region), and into the arm. It is a network of nerves passing through the cervico-axillary canal to reach axilla and innervates brachium (upper arm), antebrachium (forearm) and hand.
- 7. Horns in the spinal Cord • In the spinal cord the gray matter is present inside and white matter I towards outside while in the brain this distribution is vice versa. • On cross section of the spinal cord gray matter in spinal cord presents butterfly like structure from which some projections like “Horns” are seen, termed as • Ventral/Anterior Horn (ventral/anterior/motor root centre (Efferent Nerve) • Lateral Horn (Preganglionic sympathetic neurons, • Dorsal/posterior Horn (dorsal/posterior/sensory root centre (Afferent Nerve)
- 9. Terms to define • Ganglion: collection of the nerve cell bodies is called ganglion. E.g Dorsal root ganglion (DRG) • Ramu (Pl: Rami) Spinal nerve when exits from the vertebrae , it divides into two branches termed as, • 1. ventral/anterior primary ramus • 2. dorsal/posterior primary ramus • Ventral/anterior ramus: it is the ventral division of spinal nerve outside the vertebrae, which supplies to the skin, muscles on anterior body. • Dorsal division supplies to the skin and muscles of the back.
- 10. RTDCB • Brachial plexus comprises of Root, Trunk, Division, Cord and peripheral Branches. • A mnemonic for remember the region of the brachial plexus is: • Real - Roots • Teenagers - Trunks • Drink - Divisions • Cold - Cords • Beer – Branches
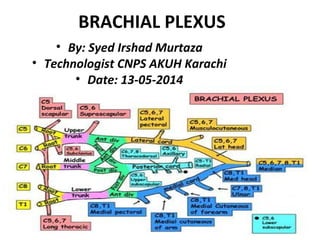
- 11. Brachial Plexus
- 12. Anatomy of RTDCB • Roots: (lying between the anterior and middle scalene muscles), • Trunks: (found in the posterior triangle of the neck), • Divisions: (lay posterior/behind the clavicle), Cords: (found in axilla & named according to their relationship with axillary/brachial artery ) & • Branches: (the five main nerve fibers in the arm).
- 14. Formation of Roots & Trunk of the Brachial Plexus The roots of the brachial plexus come from branches of the spinal vertebrae C5-8 and T1. The cervical roots, C5 and C6, fuse together to form the Upper (Superior) trunk The cervical root C7 goes on to become the Middle trunk The cervical roots, C8 and T1, fuse together to form the Lower (Inferior) trunk
- 15. The Trunks & Divisions of the Brachial Plexus • There are three trunks of the brachial plexus that lie in the posterior neck triangle. • Each of the Trunks has its two divisions • Anterior Division • Posterior Division • (Anterior divisions of the upper, middle, and lower trunks • Posterior divisions of the upper, middle, and lower trunks) • These six Divisions further unite to form the Cords.
- 16. The Divisions & Cords of the Brachial Plexus • There are two divisions of the brachial plexus that lie posterior to the clavicle. These divisions go on to form the cords of the brachial plexus. • Anterior divisions of Upper and Middle Trunks go on to form the Lateral cord • All Posterior divisions go on to form the Posterior cord • The Anterior division of the Lower Trunk goes on to form the Medial Cord
- 17. The Cords and main Terminal (Peripheral) branches of Brachial Plexus • The cords of the brachial plexus divide and join together to form the five main nerve branches of the arm. • The Lateral cord divides to become the Musculocutaneous and Median Nerve Branches. • The Medial cord divides to become the Median and Ulnar Nerve Branches • The Posterior cord divides to become the Radial and Axillary Nerve Branches
- 18. Branches from direct roots • Dorsal scapular nerve-(c4-c5)- (levator scapulae, rhomboids) • Subclavian nerve(c5-c6)- (subclavian muscle • Long thoracic nerve(c5-c7)- serratus anterior muscle • Branch from trunk • Supra scapular nerve(c5-c6)- branch from upper trunk. • Supplies infra/supraspinatus
- 19. Branches and their Roots • There are five "terminal" branches and numerous other "pre-terminal" or "collateral" branches that leave the plexus at various points along its length. • Lateral cord-1) musculocutaneous nerve(c5-c7) 2) lateral head of median nerve(c5-c7) • Medial cord-1) med.ant.thoracic nerve(c8-T1) 2) med. Cut. Nerve of arm(c8-T1) 3) med.cut. Nerve of forearm(c8-T1) 4) ulnar nerve(c7-T1) 5) med. Head of median nerve(c8-T1) • Posterior cord- 1) subscapular nerve(upper, lower)(c5-c7) 2) thoraco dorsal nerve(c5-c7) 3) axillary nerve(c5-c6) 4) radial nerve(c5-c8)
- 22. TTHHAANNKKSS