Downloaded 184 times
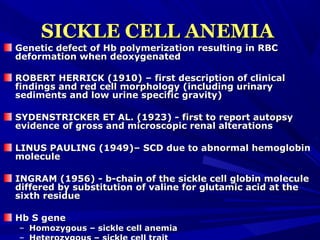
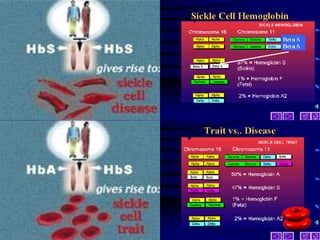
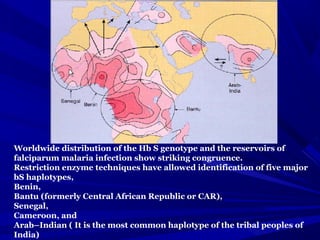
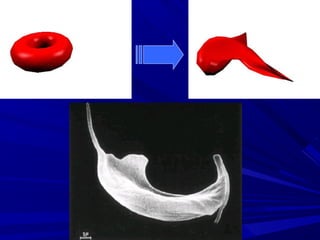
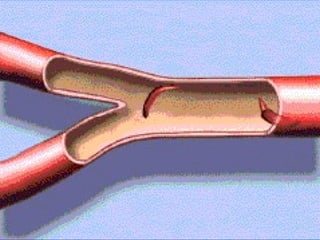
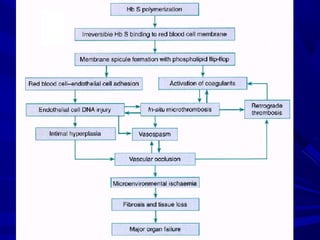
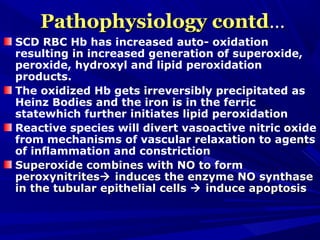
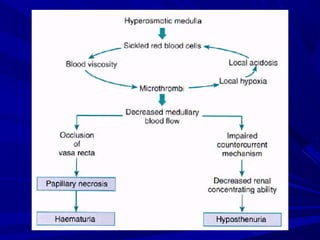
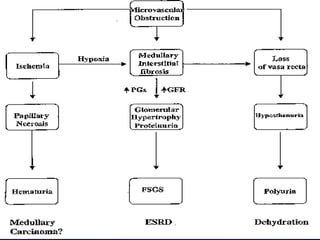


This document discusses the kidney involvement in sickle cell disease. It begins by providing background on the discovery of sickle cell disease and the genetic basis involving a mutation in the hemoglobin gene. It then covers the epidemiology and natural history of sickle cell disease, including clinical manifestations involving the kidneys. It discusses various renal pathologies seen in sickle cell disease like hematuria, proteinuria, renal papillary necrosis and chronic renal failure. Finally, it explores the pathophysiology of renal involvement, with sickling of red blood cells in the kidney vasculature and medulla playing a key role in reduced perfusion and infarction leading to chronic kidney damage.





































































































